

The following brief is part of Brookings Big Ideas for America–an institution-wide initiative in which Brookings scholars have identified the biggest issues facing the country and provide ideas for how to address them.

The first decades of the 21st century have, like the many that came before, been difficult for black America, despite the election and re-election of our first black President. There has been progress on some fronts, including narrower gaps in high school graduation rates, declining rates of teen pregnancy, and fewer suicides among black men. But the median black American will be as just as far behind their white counterpart in 2017 as they were in 2000 in terms of income, wealth, unemployment, earnings, the risk of incarceration, and many measures of health. In the last couple of decades, progress toward broader equity for African-Americans has been halting.
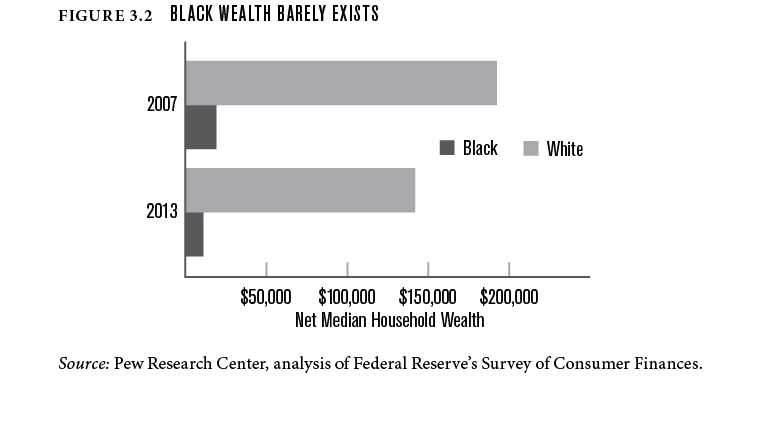
Compared to whites, black Americans face the same risk of unemployment today as in the 1960s. Between 2007 and 2013, the net wealth of the median black household fell from 10 percent to 8 percent of median white household wealth, largely the result of the differential impact of the Great Recession. In other words, the median white household now has a net wealth 13 times greater than the median black household. In 2000 the median black household had an income that was 66 percent of the median white household income. In 2015 that figure was 59 percent.
In other words, the median white household now has a net wealth 13 times greater than the median black household.
In terms of housing and health, the two areas we focus on here, the race gap faced by black Americans remains wide and stubborn. It is perhaps no surprise that black and white Americans have starkly different views on progress toward racial justice. Nine in ten blacks say African-Americans have not achieved equality in this country. Four in ten are skeptical that they ever will. Yet thirty-eight percent of white Americans think “our country has made the changes needed to give blacks equal rights with whites.” Among the half of whites that think there is more to do to achieve equality, almost all think that it will be achieved. The two groups are, as the Pew Research Center puts it, “worlds apart.”
Many of the barriers blacks face are the result of invisible, insidious force of unconscious bias. Whether it is water quality in Flint, school quality in Ferguson, environmental hazards in Dickson, Tennessee, or the inferior health care that the majority of black patients receive nationwide, the African-American experience is different, and is allowed to be different, more than would ever be accepted within white communities. Racial injustice and inequality is a problem not just for poor and low-income blacks, but for moderate-income blacks as well, as we will show. Racism, even if unintentional, determines where, how, and how well black people live, relative to other groups in America. For most African-Americans, in addition to the tangible inequalities captured in statistics, the intangible experience of being black in America is nothing like the experience of being a white person. Racial injustice lies not only in hard facts, but also in “the thick of everyday life.”1
During his presidential campaign, Donald Trump appealed directly to whites, especially those who felt threatened by immigration, trade, and diversity. His choice of words and his choice of advisers have not suggested that the inequalities faced by black Americans are at the top of his agenda. He did point out, however clumsily, the difficulties that many blacks living in cities face in finding jobs or decent schools. If the new administration decides to treat the race gap seriously, there is much that can be done, right now.
Residential Segregation: The Problem
More than half of black or white residents in 70 of the 100 largest U.S. metro areas would need to move to a different census tract in order to integrate the metro. At the rate of progress we’ve seen since the 70s, 268 of our metro areas will not be integrated until the year 2120.2 Younger black city-dwellers (born between 1985 and 2000) are just as likely to live in a high-poverty neighborhood as the previous generation (born between 1955 and 1970). White Americans are also more segregated from black Americans than from either Asian or Hispanic Americans, according to analyses by our Brookings colleague William Frey:
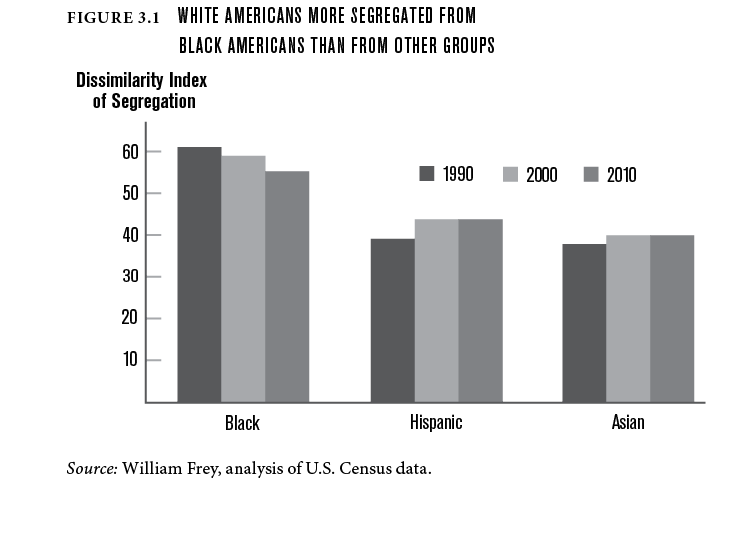
American neighborhoods have become more diverse in the last 20 years, but the main reason for this is the growth of the Asian and Hispanic-American populations, rather than significant movement by either black or white Americans. Native-born black Americans experience levels of urban neighborhood segregation nearly three times higher than native-born black British citizens.
Native-born black Americans experience levels of urban neighborhood segregation nearly three times higher than native-born black British citizens.
The causes of residential segregation are complex, enduring and overlapping. It is only a few decades since racial segregation was an explicit goal of public policy.3 But even after the successes of the civil rights movement, a number of factors continued to contribute to segregation—and, in many cases, do so still today. Four stand out:
1. Zoning. Even in the post-civil rights era, many forms of land use regulation have perpetuated segregation. Complex webs of covenants and zoning ordinances across U.S. cities—in particular for low-density development—superimposed on already highly-segregated neighborhoods, have slowed integration. When there are wide economic gaps by race, as we have in the U.S., exclusionary land-use policies based on families’ economic circumstances entrench racial segregation.
2. Transportation. Highways and runways have often damaged or cut off black neighborhoods. “Highways cut the heart out of poor areas,” as Transportation Secretary Anthony Foxx observed. Meanwhile public transit investments often fail to connect minority communities to opportunities for education and employment.
3. ‘Steering.” Black and other minority homebuyers and renters receive different treatment from realtors and agents. In 2012, white and black “homebuyers” (in fact actors) were sent to 8,000 randomly selected realtors. Black home-seekers were shown 18% fewer homes. There are some signs that realtors “steer” by race with reference to local schools.
4. Credit. After being denied home loans before the civil rights era, black Americans have continued to be denied affordable credit, and have been pushed towards sub-prime loans.4 SunTrust, Wells Fargo, and Bank of America have in recent years settled with the Justice Department (for $21 million, and $175 million, and $335 million respectively) for pushing black homebuyers into subprime mortgage deals, overcharging them for home loans, and other breaches.
5. Attitudes. Although harder to pinpoint, the attitudes and preferences of individuals and families likely plays a role too. Attitudes are shifting, but remain heavily influenced by race. Many white Americans strongly prefer to live with only a minority of black neighbors, up to roughly 20 percent of the neighborhood. Black Americans, meanwhile, prefer “50-50” neighborhoods, and are averse to homogeneous neighborhoods.5
Physical segregation by race is costly to society simply in terms of race relations. It is harder to foster an equal, tolerant, multi-racial society when people of different races live in their own enclaves. But there are more tangible costs, too, especially in terms of wealth disparities, educational opportunities, concentrated poverty and neighborhood effects, with implications for well being and health.
Wealth. The median black family has barely any wealth, in large part because blacks have not been able to participate in the wealth-generating momentum of the heavily-subsidized housing market. Many blacks who did get a foothold before the recession fell backwards during the Great Recession, when black median household wealth almost halved from $19,200 in 2007 to $11,000 in 2013. The median wealth of white households is now 13 times greater than for black households—the largest gap in a quarter century (see figure 3.2).
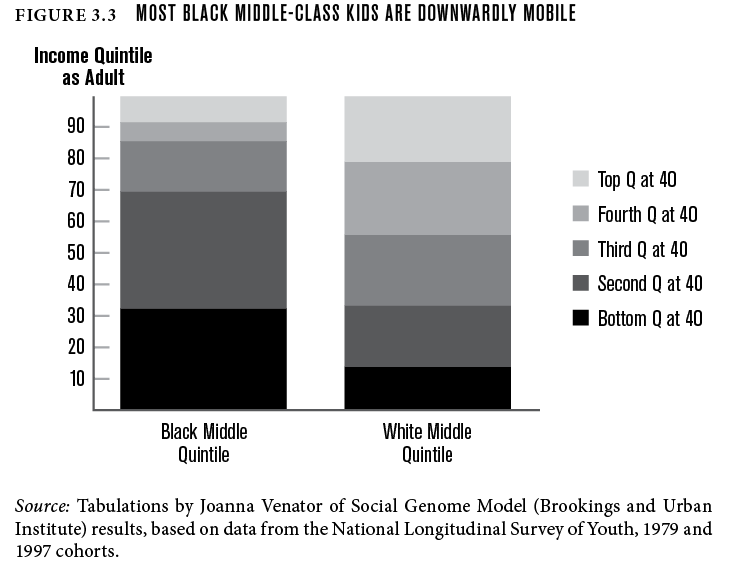
Education. There are wide, well-documented race gaps in educational outcomes. School quality is a significant factor here, and since schools tend serve specific areas, residential segregation leads to school segregation, along both racial and economic lines. The compounding effects of wealth, race and place means that even middle-income black students are more likely to attend high-poverty schools, as recent research by Sean Reardon, Demetra Kalogrides and Kenneth Shore shows. This may be one reason why black children born into middle-income families are twice as likely to be downwardly mobile as middle-income whites (see figure 3.3).
Neighborhood effects. People living in areas with higher rates of poverty have worse outcomes across a range of social and economic measures. From sidewalks to social capital, differences in safety and neighborhood quality lead to differences in outcomes, as the case-studies jointly produced by the Community Affairs Offices of the Federal Reserve System and Brookings show. Children in poor families that were able to use a voucher to move to a low-poverty neighborhood saw a 16 percent increase in college attendance and were much less likely to become single parents, compared to a control group; those who moved earned 31 percent more in their mid-twenties.
Residential segregation in terms of race is deep, and damaging. What can be done?
Residential Segregation: some solutions
A complex and enduring problem like segregation will not be solved quickly or easily. It will require sustained political attention and policy efforts from federal and local government. The president’s role may seem limited at first. But there is plenty that she or he can do, even without new laws or funds. Many of the powers needed to make progress already exist; they simply need to be used. Below we sketch out a concrete policy reform, one element of a wider strategy to tackle segregation. But the most important ingredient is political leadership—from the new President, but also from the people that she or he appoints to critical roles in the administration.
Bring back Romney (The other one)
All of these proposals will require leadership from the new President. But it will also require bolder action from HUD. Leadership of that Department is critical. We need another Romney. George Romney, that is.
“Some white people and public officials will advocate the return to state’s rights as a way to legalize segregation,” he said in the wake of the 1967 race riots: “As citizens of Michigan, as Americans, we must unhesitatingly reject all these divisive courses.” He then enacted a statewide fair housing law and told voters he wanted to end local zoning where it facilitated segregation and evenly distribute affordable housing around metro areas.
Appointed Secretary of HUD by Nixon, Romney didn’t hesitate to use the tools at his disposal—and which are still at HUD’s disposal. As Nikole Hannah-Jones reported for ProPublica:
“Romney ordered HUD officials to reject applications for water, sewer and highway projects from cities and states where local policies fostered segregated housing…[he saw his goal as using] his power as secretary of Housing and Urban Development to remake America’s housing patterns, which he described as a “high-income white noose” around the black inner city…HUD terminated grants to the Boston, Baltimore and Toledo metro areas after they rejected low-income housing slated for white neighborhoods, and won concessions.”
Since the end of Romney’s HUD tenure in 1972 there have been only a handful occasions when the department cut funding to recipients for violating the Fair Housing Act of 1968. “HUD has sent grants to communities,” wrote Hannah-Jones, “even after they’ve been found by courts to have promoted segregated housing or been sued by the U.S. Department of Justice.”6Scale up “Small Area Fair Market Rents”
In many metro areas, HUD benchmarks the value of housing vouchers to costs in the entire metro. This means voucher holders can’t afford to rent in more expensive, opportunity-rich neighborhoods, and are effectively pushed into neighborhoods with cheaper housing.
In some places, like Dallas, voucher amounts are indexed to zip codes, rather than entire metro areas. This means the allowance falls slightly in lower-rent areas, but rises in higher-rent areas. In a recent study of this “small area fair market rent” (SAFMR) approach in Dallas, Robert Collinson and Peter Ganong find that SAFMR led voucher families to enter neighborhoods with less poverty and violent crime. Across five SAFMR demonstration sites, the total cost of the program actually fell by 5 percent between 2012 and 2014. This doesn’t mean that SAFMR will make sense everywhere, but HUD should permit and encourage more cities to adopt the approach, especially in those areas with concentrated poverty.
Expand Mobility Counseling
Opening up broader, regional markets for voucher recipients will help to create more integrated cities; a powerful complement would be “mobility counseling” that helps voucher holders find a new residence. In Chicago, the Housing Opportunity Program offers a range of services, including housing search counseling and unit referrals, free credit reports, financial counseling, transport to potential new homes, expedited HUD Quality Standards inspections, legal workshops, and post-move support and house visits. The program helps families move to lower-poverty neighborhoods, according to longitudinal research, including a 2005 analysis by Mary Cunningham and Noah Sawyer. Recent analysis of the Baltimore Mobility Program suggests that families who get this kind of extra support raise their neighborhood and school expectations, and move to areas with higher-quality schools.
Health Inequality: the problem
As the new administration and Congress design the ACA replacement,7 it is important to remember that increased access is necessary but not sufficient to close morbidity and mortality gaps between blacks and whites. Health disparities resulting from racial inequity will persist as long as our nation continues to tolerate a separate and unequal health care system for black Americans.
The infant mortality rate for black babies is more than twice that for whites.This gap persists as the mother’s’ education and income rises.8 Babies born to well educated, middle-class black mothers are more likely to die before their first birthday than babies born to poor white mothers with less than a high school education:9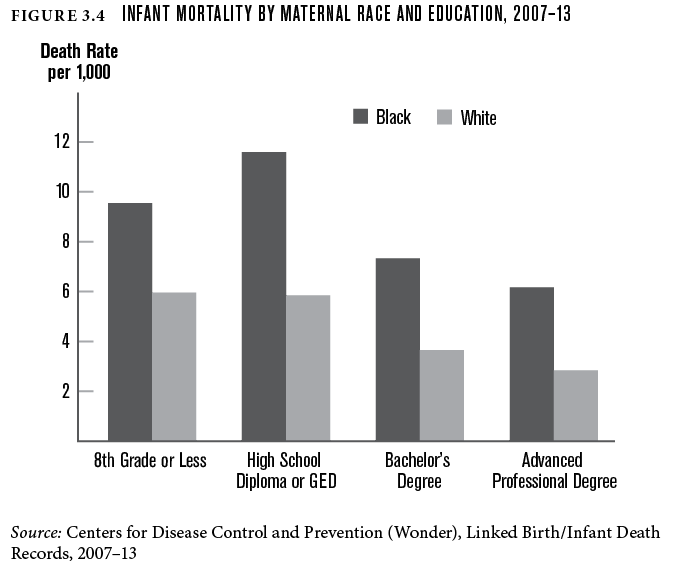
These disparities continue into adulthood. Black men still have the shortest life expectancy of any other group in America. Racial inequities, compounded by education gaps, have a cumulative negative impact on health outcomes. White men and women with college degrees live an average of 14.2 years and 10.3 years longer than black men and women with less than a high school education.10
African Americans are disproportionately treated at health care facilities with the fewest technological resources, the most poorly trained professionals, and least experienced clinicians serve predominately black patient populations.11 The most highly trained professionals serve predominately white populations.12 When compared to whites, black patients are referred to see specialists less often, receive less appropriate preventive care such as mammography and flu vaccines, receive fewer kidney and bone marrow transplants, receive fewer antiretroviral drugs for HIV, receive fewer antidepressants for diagnosed depression, and are admitted less often than whites for similar complaints of chest pain.13 No single cause explains these disparities, but five stand out.
1. Unintended race discrimination. The next president should take direct aim at the problem of unintended racial discrimination—also known as implicit bias—in medical care. Practices and policies that are race-neutral on their face actually result in inferior quality of and access to health care for blacks as compared to whites across geographic regions, diseases, facility types, and treatments.14 Though different from intentional racism, the impacts of unintended discrimination are equally harmful. Because implicit bias is subtle and hidden, it allows discrimination in health care to persist although most Americans reject explicit racism.152. Social determinants of health. The next administration must also address racial disparities in the social determinants of health. These are the conditions in which Americans live, work, and play—including access to clean, safe, affordable house and health food choices. Health care alone accounts for only 10 percent of health outcomes. Social and environmental factors (20 percent), genetics (30 percent), and behavior (40 percent) all have a greater influence on health than health care. Closing the gap in health outcomes for blacks and whites means addressing inequity in upstream social and environmental factors that impact health.
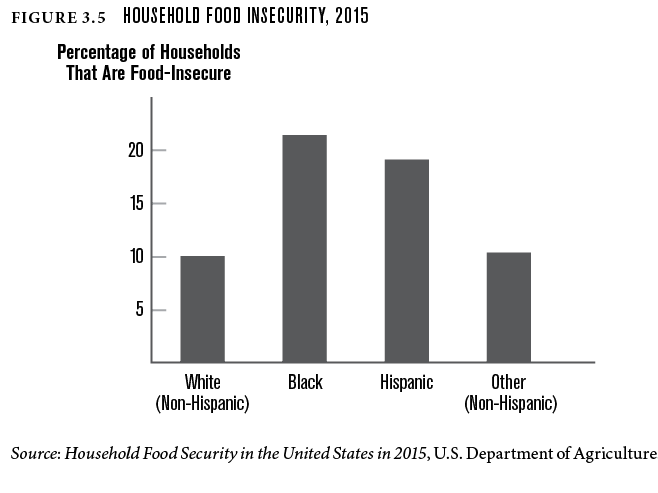
3. Housing disparities. Housing inequity is an obvious place to start. Substandard housing conditions such as pest infestation, lead paint, faulty plumbing, and overcrowding disproportionately affect black families and lead to health problems such as asthma, lead poisoning, heart disease, and neurological disorders. Blacks are 1.7 times more likely than the rest of the population to occupy homes with severe physical problems.16 Concentrated housing inequity also disproportionately exposes black communities to environmental pollutants17 and isolates black populations from essential health resources such as improved recreational spaces; quality pharmacies, clinics, and hospitals; and healthy food options (see figure 3.5).184. Health behaviors. Addressing housing disparities will encourage healthy behaviors. For example, reducing neighborhood violence and improving built environments will reduce sedentary behavior. Reducing the ratio of fast food and liquor outlets to healthy food options will reduce disparately unhealthy food consumption.19
Related Books
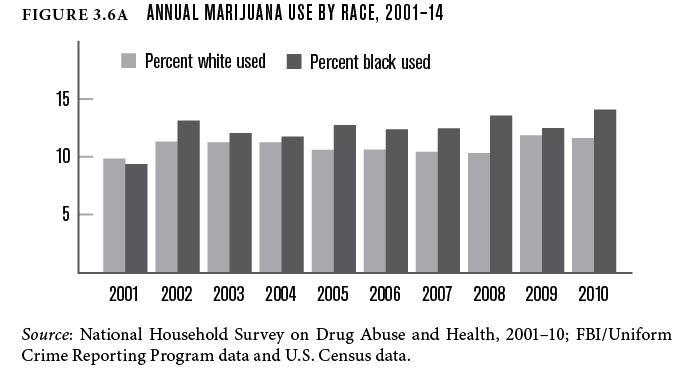
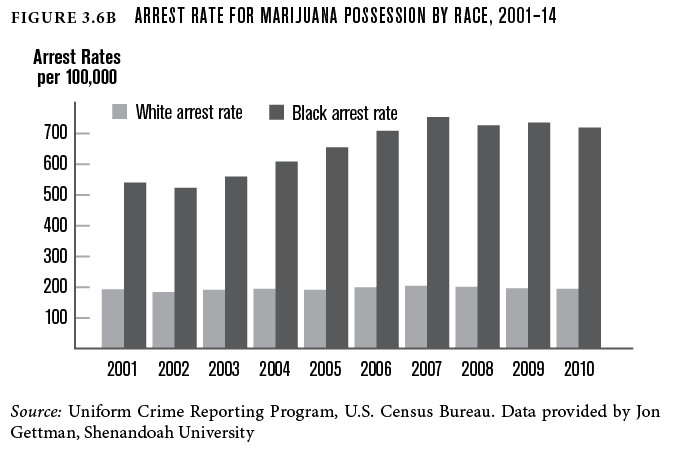
5. Criminal law enforcement. The next administration can improve health equity by addressing instances of discriminatory law enforcement that disproportionately affect black communities. Black men and women are more likely to be arrested, charged, and convicted of crimes than whites who commit the same crimes (see figure 3.6);20 disparate marijuana arrests are exemplary.21 Once convicted, black men receive prison sentences that are nearly 20 percent longer than white men for similar crimes.
The public health impact on black communities is staggering. Crowded living conditions in prisons increase transmission of infectious disease such as tuberculosis, viral hepatitis, and sexually transmitted diseases. The prevalence of mental illness and injection drug use among incarcerated populations is significantly higher than in the community at large. When prisoners are released, they bring a higher incidence of disease back to the detriment of the entire community’s health.22
Incarceration affects the mental and physical health of communities left behind. Family members experience increased mental illness such as depression and anxiety disorders, and there is an increased risk of poverty and homelessness.23 These health consequences are multi-generational. Incarceration, for example, is associated with a 30 percent increase in infant mortality.24
While there are some who express doubt that discrimination in the health care system is a cause of health disparities,25 the costs of differences in black and white health outcomes are indisputable:
1. Excess deaths. In 2005, former surgeon general David Satcher estimated the cost in terms of lives lost due to racial discrimination in health care. He concluded that over 83,000 African American men and women needlessly lose their lives yearly due to unjust and avoidable differences in the quality and quantity of health care that they receive compared with the rest of the U.S. population.26
2. Preventable hospitalizations. A Centers for Disease Control and Prevention study estimated that if black Americans had the same adjusted rate of preventable hospitalizations as non-Hispanic whites from 2004 to 2007, the African American population would have had 430,000 fewer hospitalizations.27
3. Dollars. It is estimated that racial and ethnic disparities cost Americans $1.24 trillion between 2003 and 2006.28
Health Inequality: some solutions
The new President’s most important step to achieve health equity will be to provide strong political leadership on this issue from day one. The President must publicly name the elimination of health inequality as a top priority of the new administration. This will intentionally and comprehensively re-focus the entire federal government’s attention on the issue of racial discrimination, which gave rise to the civil rights statutes beginning in 1866; but the promise of equality of opportunity has yet to be fulfilled. Hence, black Americans have suffered the worst health outcomes of any group throughout this nation’s history. We make three further recommendations:
The new President’s most important step to achieve health equity will be to provide strong political leadership on this issue from day one.
Maintain Strong Agency Leadership Committed to Health Equity
The new president must ensure that political leaders are committed and empowered to fight health inequity to the full extent of the law. This must be true throughout the federal family, and especially so for Dr. Tom Price and Scott Pruitt, the people who will occupy the positions of secretary of health and human services (HHS) and administrator of the Environmental Protection Agency (EPA). Similarly, political leadership in both agencies’ offices of general counsel and offices of civil rights must be individuals charged by the president and demonstrably committed to make the elimination of health disparities a top administration priority.
Make Efficient Use of Interagency Working Groups
Without any additional federal expenditures, the new president can strengthen the use of the Federal Interagency Health Equity Team to develop strategies, technical assistance tools, and accountability measures that will ensure that all federal agencies and departments, as well as all recipients of federal financial assistance, comply with health civil rights statute Section 1557.29
Section 1557 and its accompanying regulations provide powerful enforcement tools for the federal government to prohibit discrimination on the basis of race by health programs and activities. However, despite the strong final rule implementing the statute, Section 1557 is underutilized against racial health inequity. Currently, no sample or reported cases involving use of this statute to combat race discrimination in health care appear on the HHS website. The president can use existing interagency working groups to significantly enhance deployment of Section 1557 as a weapon against racial discrimination—whether conscious or unconscious—that produces health disparities.
Fully Implement Executive Order 12898
More than two decades have passed since President Bill Clinton signed the historic Executive Order 12898 on Environmental Justice, yet the order has not been fully implemented. The new president has an opportunity to live up to the promise that in America, “no matter who you are or where you come from, you can pursue your dreams in a safe and just environment.”30 Improving Title VI civil rights enforcement is the place to start. Currently, the EPA dismisses or rejects over 90 percent of Title VI complaints, takes an average of 350 days to complete jurisdictional reviews,31 and has never in its history made a formal finding of discrimination. The EPA has never denied or withdrawn financial assistance from a recipient. And the agency’s civil rights office has cases on its Title VI docket that were filed more than 10 years ago.32 Making the promise of this executive order a reality will help reduce health disparities suffered by black Americans.
In sum, the new president can, by reducing the inequality that separates blacks and whites, not only improve economic growth, social mobility, health, and opportunity for many, but also ensure justice for all Americans.
Authors


-
Footnotes
- This is a phrase used, in a different context, by Gerry Cohen in his book If you’re an egalitarian how come you’re so rich?
- Here, “integration” means that each census tract’s demographics match those of the larger metro. This 2120 figure assumes that more integrated metropolitan areas would experience additional integration at historical rates, which isn’t how things have played out in the past.
- See, for example, racist lending practices within the Federal Housing Administration during the 20th century.
- Redlining furthered segregation, and continues today; see here and here. Here is a list of examples of redlining in the past few years. Another example: Wisconsin’s largest bank, Associated Bank, just settled with HUD over discriminatory lending. Now they have to finance $200 million in home loans in minority census tracts, fork over $10 million in down-payment assistance, open four new offices in minority neighborhoods, and spend $1.4 million on marketing to these underserved communities.
- See here and here. Even fairly small differences in the kinds of communities people prefer to live in can have significant aggregate effects, as Thomas Schelling’s work famously showed, especially in his book Micromotives and Macrobehavior.
- One example Hannah-Jones provides: “New Orleans…. has continued to receive grants after the Justice Department sued it for violating that Fair Housing Act by blocking a low-income housing project in a wealthy historic neighborhood.”
- The Department of Health and Human Services reports that the uninsured rate among black non-Hispanics dropped by more than 50%, from 14.3% to 7.0% because of the Affordable Care Act. http://www.hhs.gov/about/news/2016/03/03/20-million-people-have-gained-health-insurance-coverage-because-affordable-care-act-new-estimates
- Lindy Washburn, “Medical Mystery Endures: Black Babies at Twice Risk of Whites for Death, Study Indicates,” Medical Press (March 2, 2011) (available here: http://medicalxpress.com/news/2011-03-medical-mystery-black-babies-whites.html).
- Laudan Y. Aron, (August 26, 2013) “Despite Fifty Years of Improvements in Infant Mortality, Large Black-White Gap Remains Unchanged,” Urban Wire: Poverty, Vulnerability and the Safety Net. (available here: http://www.urban.org/urban-wire/despite-fifty-years-improvements-infant-mortality-large-black-white-gap-remains-unchanged).
- S. Jay Olshansky, et al., (2012). Differences in Life Expectancy Due to Race and Educational Differences are Widening, and Many May Not Catch Up, Health Affairs 31(8):1803-1813.
- Justin B. Dimick, et al., (2013). Black Patients are More Likely to Undergo Surgery at Low Quality Hospitals in Segregated Regions, Health Affairs (Millwood)< 32(6):1046-1053; Laurent G. Glance, et al. (2013).
- Popescu, (2011). Differences in Admitting Hospital Characteristics for Black and white Medicare beneficiaries with Acute Myocardial Infarction. Circulation 123(23):2710-2716 (Differences in hospital quality, which may be due in part to zip code differences, may contribute to disparities).
- Kevin Fiscella and others, “Inequality in Quality: Addressing Socioeconomic, Racial, and Ethnic Disparities in Health Care,” JAMA 283, no. 19 (2000), 2579–84.
-
U.S. Department of Health and Human Services, “2015 National Healthcare Quality and Disparities Report and 5th Anniversary Update on the National Quality Strategy,” AHRQ Publication no. 16-0015 (Rockville, Md.: Department of Health and Human Services, April 2016).
- Bianca DiJulio and others, “Kaiser Family Foundation/CNN Survey of Americans on Race” (Washington, D.C.: Kaiser Family Foundation, November 2015).
- James Krieger and Donna L. Higgins, “Housing and Health: Time Again for Public Health Action,” in Urban Health: Readings in the Social, Built, and Physical Environments of U.S. Cities, edited by H. Patricia Hynes and Russ Lopez (Burlington, Mass.: Jones and Bartlett Publishers, 2009), 106.
- Liam Downey and Brian Hawkins, “Race, Income, and Environmental Inequality in the United States,” Social Perspectives 51, no. 4 (2008): 759–81.
- R. Williams and C. Collins, “Racial Residential Segregation: A Fundamental Cause of Racial Disparities in Health,” Public Health Report 116, no. 5 (2001): 404–16.
- Angela Hilmers, David C. Hilmers, and Jayna Dave, “Neighborhood Disparities in Access to Healthy Foods and Their Effects on Environmental Justice,” American Journal of Public Health 102, no. 9 (2012): 1644–54.
- Dylan Matthews, “The Black/White Marijuana Arrest Gap, in Nine Charts,” Washington Post Wonkblog, June 4, 2013.
- Sandro Galea, “Incarceration and the Health of Populations,” Boston University School of Public Health, March 22, 2015, www.bu.edu/sph/2015/03/22/incarceration-and-the-health-of-populations/.
- Editorial Board, “Mass Imprisonment and Public Health,” New York Times, November 26, 2014.
- Christopher Wildeman, “Imprisonment and (Inequality in) Population Health,” Social Science Research 41 (2011): 74–91.
- Jonathan Klick and Sally Satel, The Health Disparities Myth: Diagnosing the Treatment Gap (Washington, D.C.: American Enterprise Institute Press, 2006).
- Joe Palazzolo, “Racial Gap in Men’s Sentencing,” Wall Street Journal, February 14, 2013.
- David Satcher and others, “What If We Were Equal? A Comparison of the Black-White Mortality Gap in 1960 and 2000,” Health Affairs 24, no. 2 (2005): 459–64.
- Carrie Hanlon and Larry Hinkle, “Assessing the Costs of Racial and Ethnic Health Disparities: State Experience” (Rockville, Md.: Health Care Cost and Utilization Project, June 24, 2011).
- Thomas A. LaVeist, Darrell J. Gaskin, and Patrick Richard, “The Economic Burden of Health Inequalities in the United States” (Washington, D.C.: Joint Center for Political and Economic Studies, 2009).
- See, for example, Executive Order 11246, as amended by Executive Orders 113575 and 10286 and applicable regulations.
- See, for example, Lisa Garcia, “President Obama’s Proclamation on Environmental Justice,” EPA blog, February 25, 2014, https://blog.epa.gov/blog/tag/executive-order-12898/.
- Editorial Board, “The E.P.A.’s Civil Rights Problem,” New York Times, July 7, 2016.
- U.S. Commission on Civil Rights, “Environmental Justice: Examining the Environmental Protection Agency’s Compliance and Enforcement of Title VI and Executive Order 12,898” (Washington, D.C.: September 23, 2016).
U.S. Department of Health and Human Services, “2015 National Healthcare Quality and Disparities Report and 5th Anniversary Update on the National Quality Strategy,” AHRQ Publication no. 16-0015 (Rockville, Md.: Department of Health and Human Services, April 2016).
The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).


