If it was not clear before COVID-19, it is obvious now that achieving the United Nations 2030 Sustainable Development Goals and the World Health Organization’s Triple Billion Goals will be impossible without universal health coverage (UHC). UHC is measured by the World Health Organization (WHO) along three dimensions: population coverage (who’s covered); service coverage (which services are covered); and financial coverage (what proportion of health service expenses are covered). With limited resources, many trade-offs must be made among these three dimensions. According to a 2017 report by the WHO and World Bank, the past decade’s increase in service coverage is disastrously paralleled with an increase in catastrophic spending. This situation forces people to choose between physical health or financial ruin, a terrible yet common decision many must make.
While there is no one-size-fits-all path to UHC, a recent study on China and Vietnam may shed light on this dilemma. Both countries have made impressive progress toward UHC in the past decade while prioritizing different dimensions. China’s prioritization of population coverage helped it achieve the largest population coverage in history in a relatively short period of time. Meanwhile, Vietnam provided a generous benefit package that is more equitable for all.
Both have made sizeable gains in population health, and other countries could learn from their struggles and successes. Our study points to three lessons.
Lesson 1: A commitment to fund national health insurance programs is the sine qua non for universal coverage
Both countries’ strong political commitment can be seen in large government subsidies for health insurance, especially for the poor and the vulnerable, and the enacting of laws, policies, and decrees to establish and promote health insurance schemes.
China established three different public insurance schemes in 1998, 2003, and 2007, each targeting a different population—urban workers, rural residents, and the rest of the urban population respectively. Currently, insurance schemes are run at the provincial/county level and there are wide disparities among the schemes. Vietnam established health insurance for employees in the 1990s, but it wasn’t until 2003 that the government began taking more financial responsibility for the poor. That was when it increased coverage, though incrementally. Both countries achieved impressive increases in population coverage over the span of 13 years through the critical policies/laws/decrees they enacted.
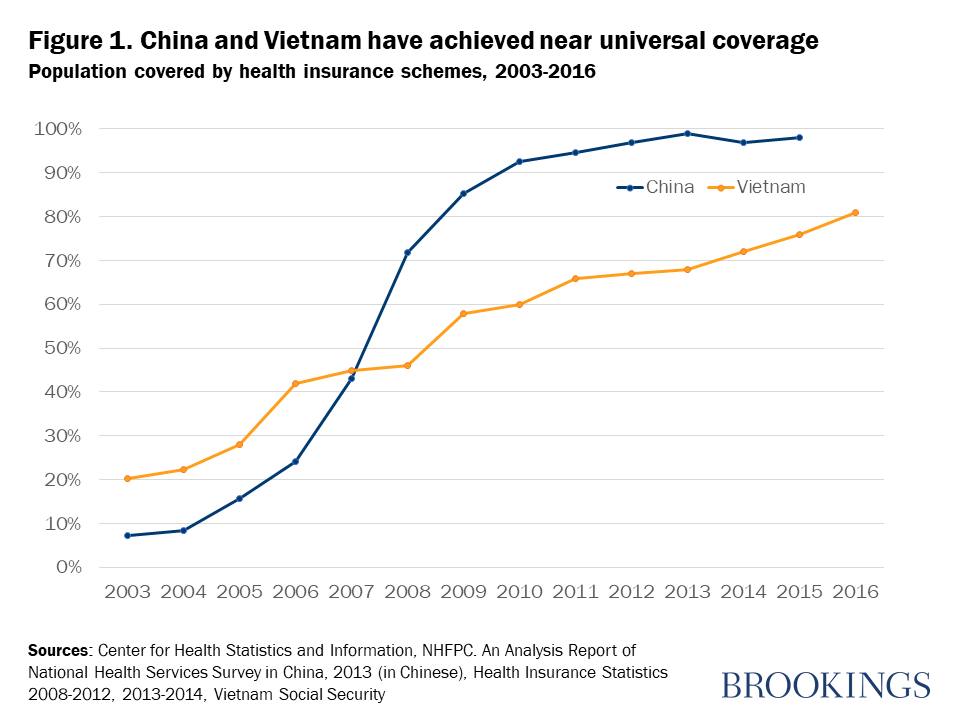
Figure 1 reports population coverage in China and Vietnam over time. The year of implementation for key policies is identified in the chart: China’s New Cooperative Medical Scheme (NCMS) in 2003 and Urban Resident’s Basic Medical Insurance (URBMI) in 2007, and Vietnam’s Health Care Fund for the Poor (HCFP) in 2003, Law on Health Insurance (LHI) in 2008, and subsequent 50 percent subsidy of the LHI for the near poor in 2009.
Lesson 2: While population coverage is the foundation of UHC, financial risk protection and healthy populations are the real goals
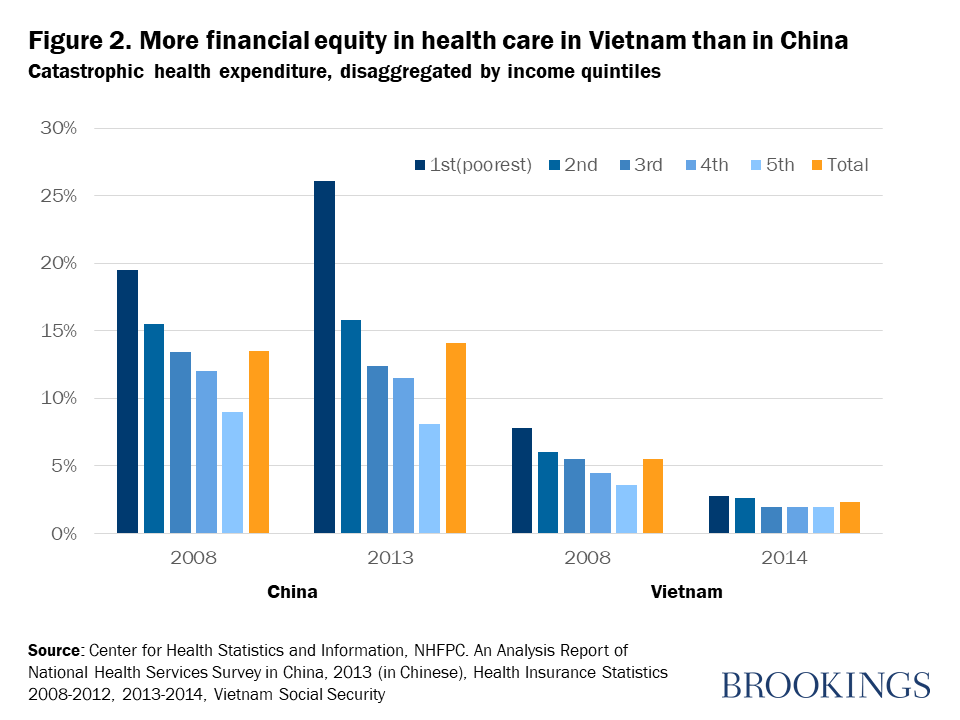
Let’s use catastrophic health expenditure (CHE)—when health spending exceeds 40 percent of non-subsistence spending for a household—as the metric to understand the importance of this lesson. While more people have insurance in China, CHE rose alongside a widening disparity between income quintiles. Meanwhile, CHE has fallen in Vietnam and the gap between the richest and poorest is decreasing (Figure 2). It is believed that rapid economic growth, an aging population, improved transportation, and improved access to health services in China have led to increased access and a willingness to pay for health services. Unfortunately, this positive development has also increased the risk of CHE for poorer families in China, a direct contradiction of UHC’s purpose. Existing perverse economic incentives given to health providers in China have worsened this situation.
Meanwhile, Vietnam’s incremental approach toward UHC focusing on the poorest and most vulnerable when growing its health insurance scheme has been seen as an equitable approach to UHC. This slower approach to population coverage has helped Vietnam decrease CHE. However, we should note that a slower approach means those left uninsured are, in the meantime, at much higher risk of CHE or unmet needs of health care. Of course, Vietnam’s pro-poor design focused on stabilizing the most vulnerable populations, so those uninsured are assumed to have some form of financial capacity.
While both countries have made incredible gains, they still have room to improve in one dimension of coverage or another. For countries aiming to achieve UHC, deciding what to prioritize and how fast to implement policy interventions should take into consideration your country’s reality, not anyone else’s.
Lesson 3: How much a society values equity determines the path it takes to UHC
Within and between countries, there have always been differences in how equity is defined and how much it is desired, and they lead to differences when developing health systems. While differences regarding equity are not inherently negative, they are part of why achieving UHC can be difficult.
We can see these differences play out when we examine which dimensions countries prioritize as they strive for UHC, like prioritizing population coverage or prioritizing service coverage. Despite China’s wider population coverage, in reality, access to health care services and financial protection are still determined primarily by geographic location and economic status. Meanwhile, in Vietnam, disparities between the economic groups and geographic locations have been shrinking. This difference can be attributed to differing priorities: China prioritized population coverage through their reforms, while Vietnam prioritized service coverage through their pro-poor design. When these countries decided on service packages for the health insurance schemes, China’s “essential package” was frugal. Meanwhile, Vietnam’s equitable package administered predominantly in the public health care system allowed it to affordably provide essential health services. The lesson: Taking your time in broadening population coverage with a strong services package might be better for your population’s health and your country’s wallet.
Recap: Commitment, clear goals, and customization
The takeaway lessons for other developing countries that want to achieve UHC through health insurance include strong political commitment with financial resources and an incremental approach that is attuned to their population. When designing health insurance systems, keeping tabs on all three UHC dimensions, ensuring consistent service coverage for essential health services, and government subsidies for vulnerable populations are needed.
Despite China and Vietnam’s progress toward UHC, they face big challenges. An aging population and shifting disease burdens are putting a lot of pressure on the financial sustainability of their health insurance systems. Cross subsidization, provider payment reform, and cost-effective benefit packages have to be carefully designed and implemented to improve the efficiency, equity, and affordability of health insurance systems. Though the future is uncertain, both China’s and Vietnam’s prospects look promising as they continue to customize their designs to their realities.
Related Content



Authors




Commentary
Getting to universal health coverage in China and Vietnam
February 3, 2021