Health experts are rightly alarmed that the world is unprepared for the next pandemic. So, when the rare and deadly Nipah virus broke out in the southern Indian state of Kerala in May, many feared that it would spread on the scale of SARS in China or Ebola in West Africa. But the authorities and the public controlled its spread. In the end, 19 people were infected and 17 died. Key to the response was Kerala’s past investments in education and health—the state ranks 10th in GDP among Indian states and territories, but first in human development.
A Nipah infection leads to acute respiratory problems and brain inflammation. The virus—of which there is no vaccine yet—was first identified in among pig farmers in Malaysia, when it killed over 100 people in 1998. Cases now appear almost yearly in Bangladesh, and there were two previous occurrences in West Bengal, India. Its containment in Kerala was impressive because this Nipah strain was more deadly and infectious than the one in Malaysia.
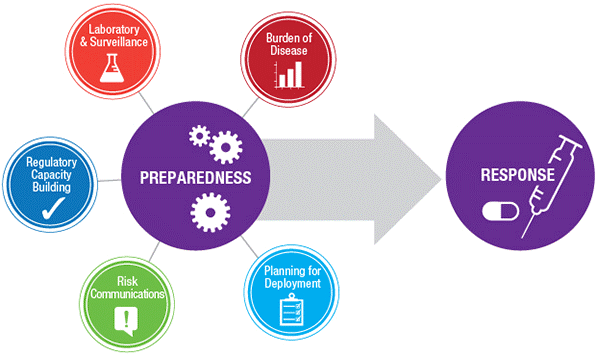
Much has been learned about the links between the degree of preparedness and the effectiveness of response to a breakout of infectious diseases. Being prepared involves vital elements ranging from laboratory surveillance to communication about the risks (Figure 1).
Figure 1: Multi-pronged Preparation and Response to Viral Outbreaks
The key to containment in Kerala was the speed of detection. With the second case, where the patient arrived at Kozhikode’s Baby Memorial Hospital on May 17, Dr. Chellenton Jayakrishnan, the attending neurologist, quickly realized that the symptoms were unlike any encephalitis cases the team had ever seen, and reminiscent of the Nipah virus analyzed in a recent neurology journal.
In the first case, the patient’s brother died 12 days earlier and his father and aunt also became infected. The patient’s samples were dispatched quickly to Karnataka state’s Manipal Centre for Virus Research (MCVR) about 300 km from Kozhikode. MCVR made the detection in a day and got a medical team into the field within 24 hours for containment and surveillance, and to alert local communities. The head of MCVR, Dr. Govindakarnavar Arunkumar, credits the timely response to preparedness, capacity building, and coordination with state, national, and global organizations.
The MCVR quickly got re-confirmation of the Nipah diagnosis from the National Institute of Virology in Pune, India before Government of India appraised the WHO of the outbreak. Within hours of the patient’s arrival at Baby Memorial, Kozhikode’s district medical officer, Mrs. V. Jayashree, put together a team of entomologists to initiate protective action at the patient’s home. The State’s Chief Minister, Mr. Pinarayi Vijayan, and Health Minister, Mrs. K.K. Shylaja took charge of actions directed at isolating patients, using surgical masks and decontaminating surfaces.
One reason the virus was contained was the relatively high proportion of doctors and nurses in Kerala, and that private spending on health is the highest in India. Kerala’s high literacy rate may not have the expected economic payoffs, as heavy regulations and labor laws have stifled growth. But its contribution to health care and participatory responses comes through in this recent experience.
The equal presence of women in the workforce enables the use of the full potential of the society’s human capital. Girls are educated as much as boys; a girl born in Kerala can expect to live to 78 years, comparable to upper middle-income countries. The line of command in the Nipah campaign included both men and women not only in senior health management but also among the doctors and paramedics involved in containing the spread of the virus.
Community spirit and societal resilience, underscored by a high degree of participatory style of governance, played a part as well. Kozhikode Medical College’s doctors, nurses, and administrators went into high gear. Notable was the mutual trust and social cohesion beyond religious divides in India’s most religiously diverse state.
Against these positives was the environmental destruction in Kerala, particularly related to garbage disposal in urban areas. Had the authorities not been able to quickly contain the virus, ecological factors would have spurred its spread. Worsening environmental degradation was connected to outbreaks of the mosquito-borne Chikungunya virus in Kerala and the Zika virus in Brazil. In both instances, reckless deforestation and urban decay played a role.
In the wake of worldwide threats of new viral outbreaks, Kerala’s experience holds lessons going forward. Disease prevention and rapid response, coupled with environmental protection, should be bigger priorities everywhere.
Related Content



Author

The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).



Commentary
Containing a deadly virus: Lessons from the Nipah outbreak in India
July 23, 2018