The Omicron wave of SARS-CoV-2 in December 2021-February 2022 caused over 30 million new cases and hundreds of thousands of deaths, with a daily death toll greater than total deaths caused by Hurricane Katrina—many more than the Delta wave. This burden fell unequally on society, with Americans over 65 representing almost 80% of the deaths and significant racial disparities.
Our new analysis suggests that many of these cases were preventable. Using a data-driven computational model, we identify specific policy strategies that would have reduced infection rates and peak level of cases during the winter surge. These critical lessons can guide preparedness moving forward as we face a potentially even larger wave in the autumn.
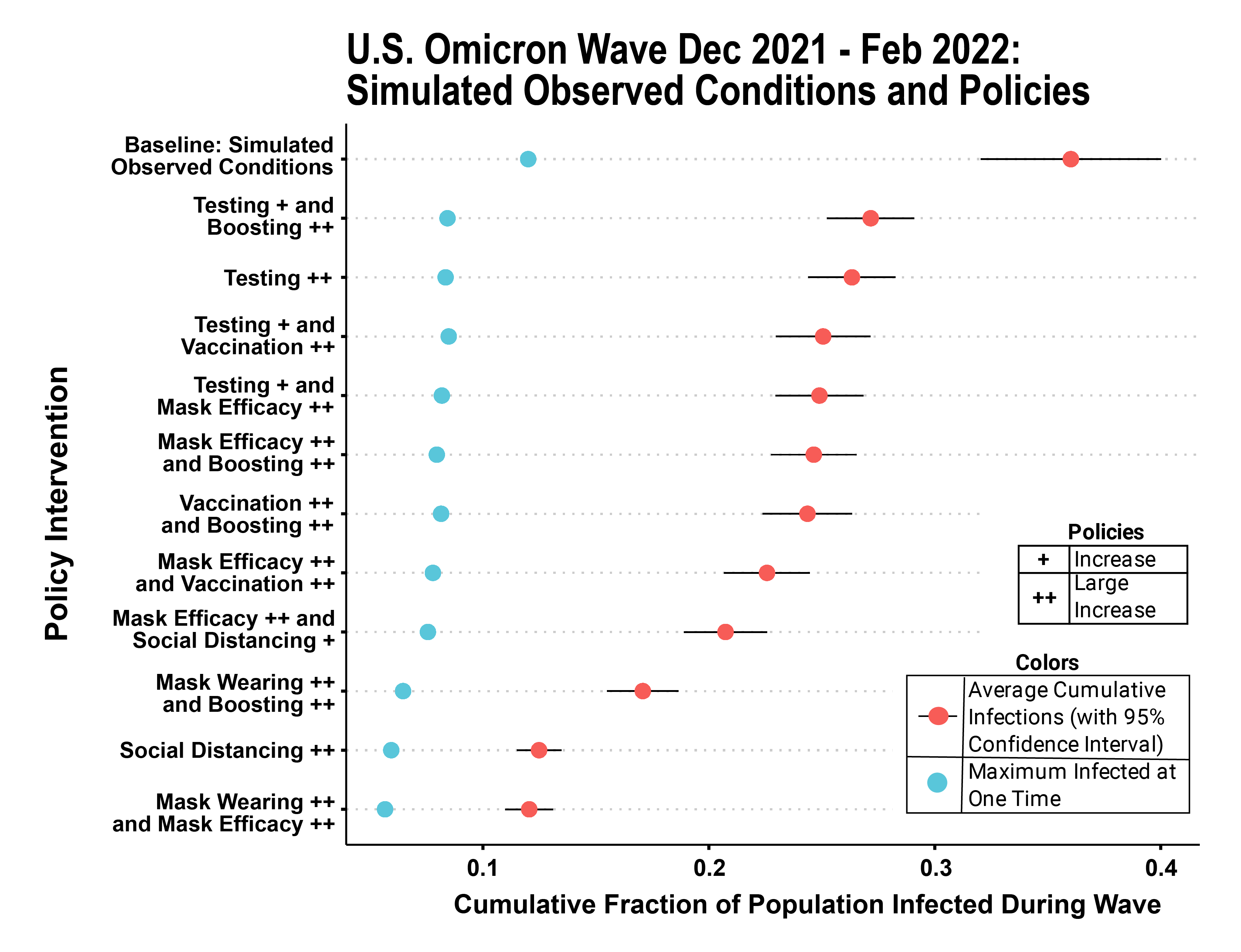
The model we used to find these results, called TRACE, was developed by a team from Brookings, Washington University in St. Louis, and the University of Vermont, building on previous work that informed early-pandemic policy nationally and locally. We considered a wide variety of potential containment strategies that could have been deployed before or during the Omicron wave and used TRACE to simulate how many cases would have occurred during each of these scenarios, allowing for us to readily compare them to one another. The model includes a wide variety of policy options: both small and large increases in testing capacity; faster rollout and uptake of vaccines; faster rollout and uptake of booster doses of vaccine; small and large increases in mask wearing; increased access to and substitution of high-quality respirators over low-quality masks; and moderate or strong social distancing policies such as school closures and remote work. Each of these actions is evaluated in isolation as well as hundreds of combinations of policy responses.
Some of our most significant findings are:
- Multiple alternative containment strategies would have resulted in substantially lower rates of cumulative infection and peak surge levels during the winter Omicron wave than those that were actually experienced. Although we do not directly estimate downstream effects, lower case rates translate to a reduction in deaths, reduced burden on the health care system, and fewer instances of long-term symptoms or downstream health consequences such as “long COVID” or immune-system driven disease risk in young children.
- A significant increase in consistent usage of high-quality masks could have reduced cases by as much as two-thirds. Although masking in the United States has been politicized and efforts to increase mask usage have been controversial, our simulations demonstrate that masking remains a very effective approach to containing spread of SARS-CoV-2. In our simulations, consistent masking by 70% of Americans during the surge would have been almost as effective as widespread closures of businesses and schools.
- A large increase in testing capacity alone could have reduced cumulative and surge infection rates by nearly one-third.
- A higher take-up rate of booster shots and earlier availability for those eligible would have reduced cumulative infection rates by up to 15% of the U.S. population during the Omicron wave. Rapid increases in vaccination for children under 18 would also have led to large decreases in disease spread. Much higher investment in uptake of boosters and vaccines, including in the youngest age groups, would likely be needed before a wave to provide a substantial dampening effect.
- Combinations of “lighter touch” responses (such as modest increases in mask usage combined with modest increases in testing) can be as powerful as intensive investment in a single policy approach and may be more practical.
A fall wave may be driven by a variant that looks different from Omicron, but our results can still inform policy investments that will save lives.
In addition to looking at the “policy counterfactuals” above (policy choices that could have been made but were not), we also used TRACE to look at “epidemiological counterfactuals” that represent how the wave might have played out if a variant even more contagious than Omicron (or one better able to evade immunity) had become dominant. Our key finding from this analysis is that, although all containment policies are less effective in absolute terms against a highly contagious or high immune-escape variants, their relative impact compared to one another is largely invariant—that is, the choice of which policies to invest in for maximum preparedness remains nearly the same. A fall wave may be driven by a variant that looks different from Omicron, but our results can still inform policy investments that will save lives.
At a time when policy focus and public attention have largely shifted away from COVID, these new results show how big a difference policy choices and preparedness investments can make. Both the analysis above and our previous work with TRACE underscore the contributions that policy simulations can continue to make to identifying robust and practical policy solutions in the face of uncertainty and rapidly changing dynamics on the ground. Models which consider a broad range of policy choices and can simulate impact across diverse interacting populations are also particularly well suited to providing guidance with respect to long-term impacts, equity implications, and linkages to health care or economic systems, as we are doing in our continued work with TRACE.
The Brookings Institution is financed through the support of a diverse array of foundations, corporations, governments, individuals, as well as an endowment. A list of donors can be found in our annual reports published online here. The findings, interpretations, and conclusions in this report are solely those of its author(s) and are not influenced by any donation.
Related Content


Authors


The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).


Commentary
How the Omicron response can prepare us for the next wave
May 25, 2022