Home | About TRACE-OMICRON | TRACE 1.0 | TRACE-STL
TRACE-Omicron
The Omicron wave of SARS-CoV-2 caused over 30 million new cases and hundreds of thousands of deaths. Results from the new analysis presented below suggest specific policy strategies that could have prevented many of these cases and identify urgent actions to prepare for a potential next wave of the pandemic.
Our analysis uses TRACE (Testing Responses through Agent-based Computational Epidemiology), an agent-based computational model developed by a team from Brookings, Washington University in St. Louis, and the University of Vermont. TRACE draws on an extensive body of epidemiological evidence about both the current and past epidemics, and it was designed to manage a high degree of remaining uncertainty about some of the parameters it uses. The version of the simulation model described here (“TRACE-Omicron”) builds upon previous work that successfully informed response strategies during the early stages of the pandemic in 2020 and localized containment while easing social distancing following the widespread availability of vaccines in 2021. In this new work, we have extended the model to generate policy-relevant lessons from the recent Omicron wave of the COVID-19 pandemic and for future preparedness. For more details on the model design, see About TRACE-Omicron.
SUMMARY OF APPROACH
Using an extended version of our model that accounts for updated science on SARS-CoV-2, features specific to the Omicron wave, and the policy context in late 2021-early 2022 in the United States, we examine a series of “policy counterfactuals” (preventative actions that might have been taken before or during the Omicron wave but were not) and “epidemiological counterfactuals” (characteristics the Omicron variant might have had but ultimately did not). Our analysis allows us to answer several important questions related to current and future preparedness:
- Which policy steps (either if taken ahead of time in preparation or as a rapid response in early 2022) might have helped reduce the size and speed of the Omicron wave, reducing the significant health consequences from this episode of the COVID-19 pandemic? How many total cases might each action or set of actions prevented? How much lower might the peak of the surge in cases have been?
- How much worse might the early 2022 wave have been if the Omicron variant had been more contagious or better at evading vaccines? Would this have changed the relative effectiveness of policy alternatives?
- What do the answers to the previous two sets of questions suggest might be important investments to make as a nation now, to prepare for a potential new variant or “fifth wave” (perhaps in the autumn)?
- What might the computational modeling approach TRACE represents tell us about other past or future epidemics and policy options?
KEY RESULTS
We considered a wide variety of potential containment strategies that could have been deployed before or during the Omicron wave—including small or large increases in testing capacity, faster rollout and uptake of vaccines, faster rollout and uptake of boosters, increased mask wearing, increased access to and substitution of high-quality respirators over low-quality masks, and moderate or strong social distancing policies such as school closures and remote work. We looked at each of these policy actions in isolation as compared to the baseline (what actually was done and what happened). We also explored hundreds of combinations of these policies in both low and high levels of investment or implementation.
Our results show substantial differences in the estimated impact of different policy regimes, with the most powerful containment policies projected to have reduced the number of new COVID-19 cases during Omicron by more than two-thirds while other intensive policy actions would have made only a moderate impact.
Figure 1 shows some of the most important of these comparisons (for full results, see forthcoming manuscript):
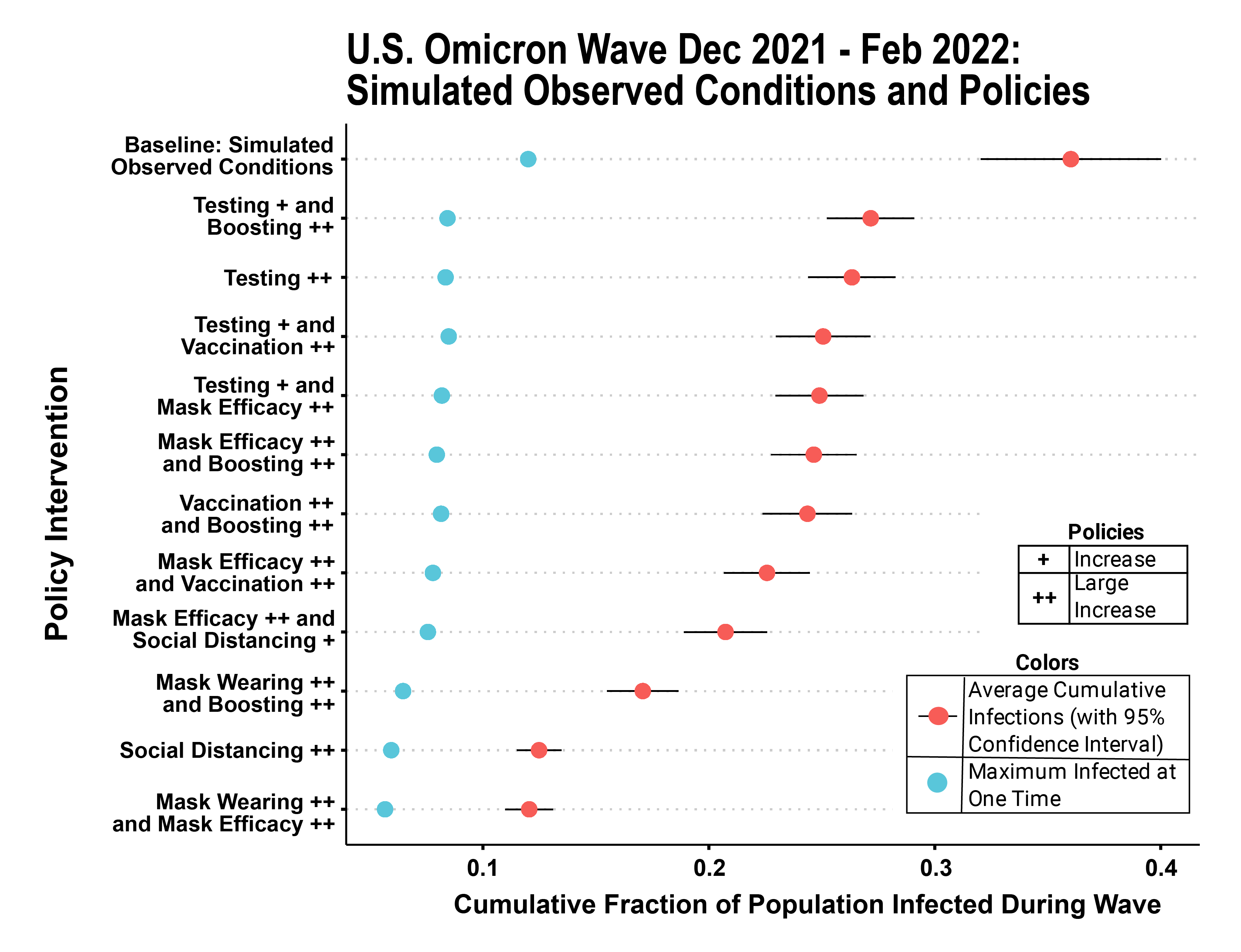
Each row of the figure represents a specific policy configuration, beginning with baseline (actual policies in place during Omicron) on the top row. Single or double ‘+’ symbols denote increases in the strength of a policy moderately (+) or significantly (++) over baseline. [For example, row 2 indicates somewhat more testing (+) combined with much higher levels of booster shots (++)]. Within the figure panel, projected total (cumulative) infections for each condition are shown with a red dot (and associated confidence interval). A separate blue dot indicates the peak surge level reached at any time in the simulated epidemic.
Some of the most important findings to emerge from the analysis summarized in Figure 1 are:
- Multiple policy options would have allowed for substantially lower rates of cumulative infection and peak surge levels during the winter Omicron wave than those that were actually experienced. This would have translated into a reduction in death, burden on the health care system, and instances of long-term symptoms or downstream health consequences (“long COVID”).
- Strong forms of individual policies in isolation (dramatic increases from baseline) were capable of reducing infections by almost two-thirds, but combinations of less intensive policies were almost as effective (and likely much less costly or disruptive).
- The greatest reductions in infection came from social distancing or significant increases in effective mask usage. Although both options would likely have faced some controversy, they could have potentially reduced cumulative Omicron infection rates in the U.S. population from over 35% to approximately 10%.
- Several other policies with less potential controversy or economic cost could have also resulted in improved outcomes; for example, a large increase in testing alone could have reduced cumulative and surge infection rates by nearly one-third.
- There is potential for “policy synergy.” Combinations of responses such as increased availability and use of high-quality (e.g., N95) masks in settings where masks were already worn, increased testing, and increased vaccination and boosting take-up would have had similarly positive impacts.
- A higher take-up rate of booster shots and earlier availability for those eligible would have reduced cumulative infection rates by up to 15% of the U.S. population during the Omicron wave. Rapid increases in vaccination for children under 18 (e.g. vaccination of this group at the same rate as adults, about 75%) would also have led to large decreases in disease spread. In looking forward to possible future waves, it might thus be advisable to consider how to substantially ramp up delivery infrastructure. Both of these policies were even more effective when combined with others (e.g., testing).
To provide a more nuanced look at the differences between policy regimes, we look more closely at two widely discussed policies: booster doses of vaccination and masking.
Figure 2 shows that substantial increases in uptake of booster doses of vaccine could have prevented infections during the Omicron wave in about 15% of the population.
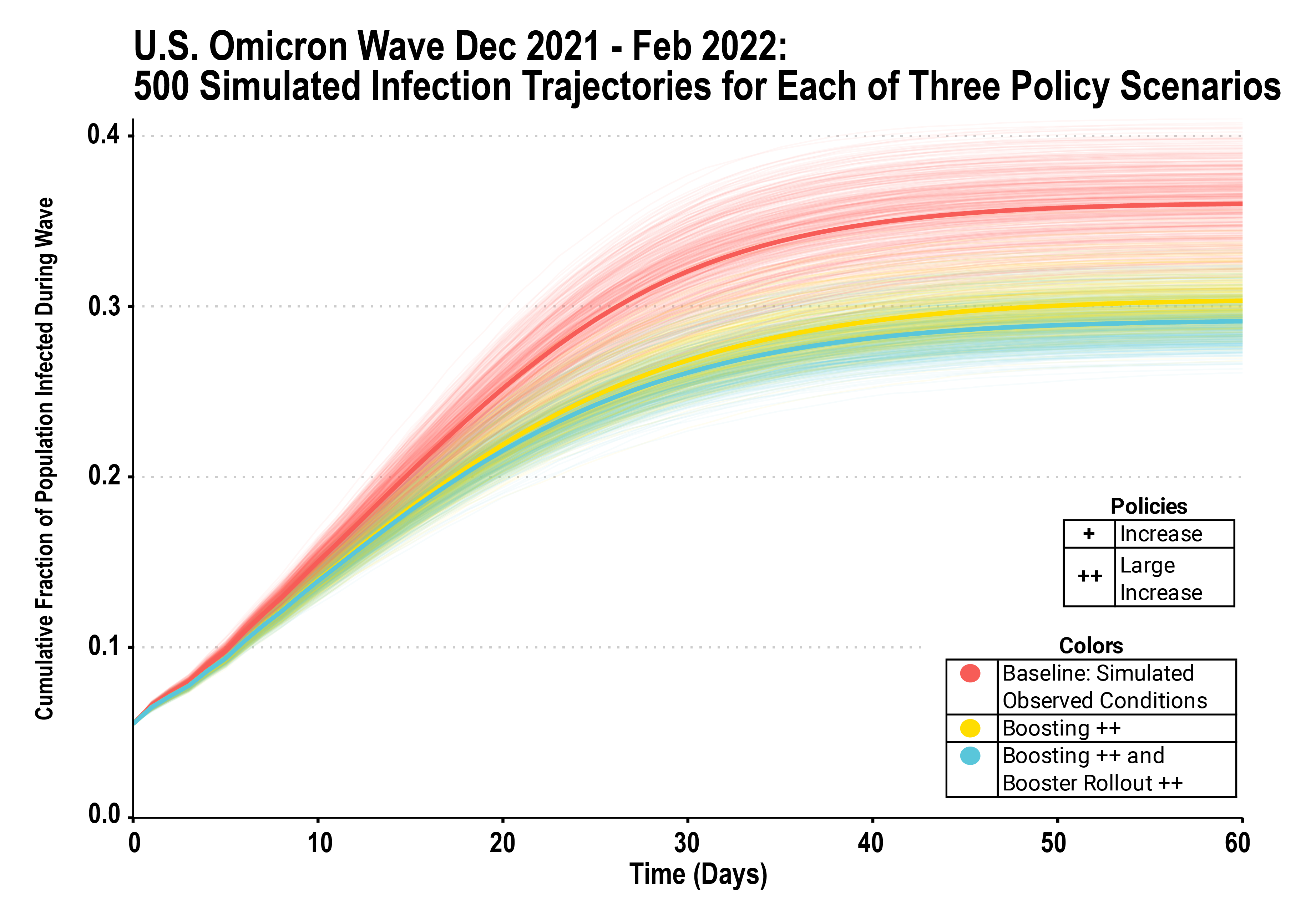
Each individual line in Figure 2 represents a single simulation with randomized initial set of infected agents, with bold lines representing the ensemble average. Red lines are the baseline; yellow lines represent a scenario in which a larger fraction of the population (47% vs 20%) had received booster doses before the end of 2021; blue lines show a scenario in which both this larger fraction had already received booster doses before the end of 2021 and an accelerated pace of ongoing rollout of boosters and primary vaccines was achieved in early 2022.
Vaccines remain a critical public health tool in managing COVID-19—and their usefulness in preventing serious disease, hospitalization, and death has been largely undiminished by Omicron. Our focus in the results presented here is on total cases of infection (and the level of transmission), which remains important as a significant fraction of even mild cases yield long-term symptoms (“long COVID”), and many Americans are not or cannot be vaccinated fully. Given new evidence about the falloff over time in protection from infection conferred by the initial vaccine series and the greater ability of Omicron to evade immunity, booster shots have been essential for providing continued population-level protection against infection (and thus spread of the virus). Figure 2 demonstrates that a faster rollout of boosters could have reduced cases, but that this alone would not have prevented the majority of cases at levels shown here. Much higher investment in uptake of boosters (beyond the 47% uptake shown here) and vaccines more generally, including in the youngest age groups, as well as potential variant-tuned boosters, would likely be needed before a wave to provide a broader dampening effect.
As shown in Figure 3, a significant increase in the fairly low levels of consistent usage of high-quality masks that were observed during the Omicron wave could have dramatically reduced cases—preventing as many as 2/3 of them—according to our TRACE simulations:
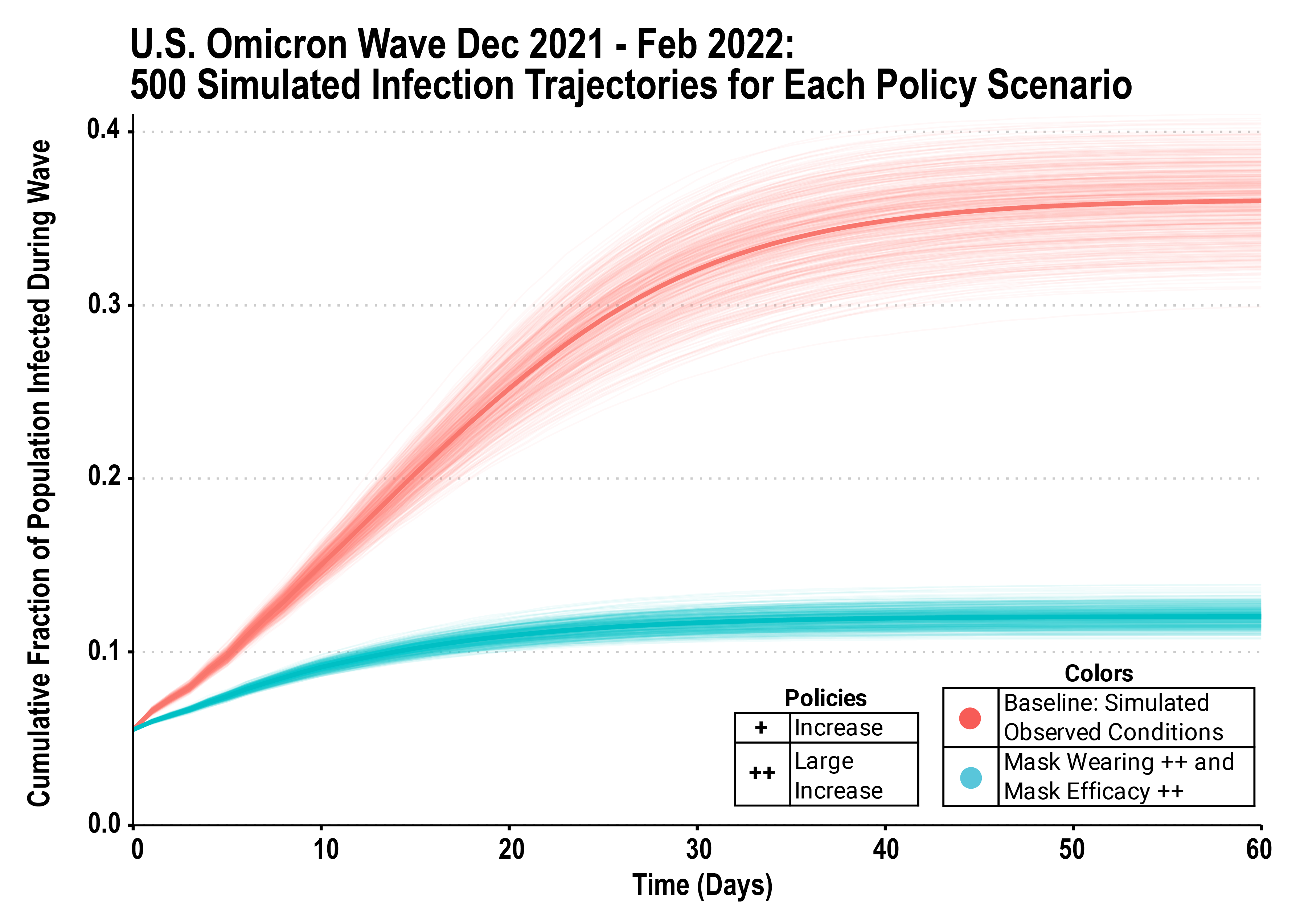
As before, each individual line in Figure 3 represents a single simulation with randomized initial set of infected agents, with bold lines representing the ensemble average. Red lines are the baseline; blue lines represent a scenario in which wearing of high-quality masks doubled to 70%. Although masking in the United States has been politicized and efforts to increase mask usage have been controversial (making such a policy strategy potentially less feasible), the simulations shown here demonstrate that it can be a very effective approach to containing spread of the virus even in the absence of other containment policies and even with a highly contagious variant such as Omicron.
ADDITIONAL RESULTS
In addition to looking at the “policy counterfactuals” above (policy choices that could have been made but were not), we used TRACE to look at how the wave might have played out differently if a different variant of SARS-CoV-2 had become dominant—e.g., one that could elude immunity more effectively than Omicron or was even more contagious. These “epidemiological counterfactuals” allow us to test how our policy results might differ against a future variant of the virus, such as could potentially arise later this year. Full results from this analysis are shown in our forthcoming manuscript. Our key finding from this analysis is that, although all policies are less effective in absolute terms against a highly contagious or high immune-escape variants, their relative impact compared to one another is largely invariant—that is, the choice of which policies to invest in for maximum preparedness remains nearly the same. The differences between policies are, in many cases, accentuated; for example, rapid deployment of masking or distancing is even more effective relative to testing and vaccination against variants that evade immunity. Similarly, testing and vaccination investments together are much more powerful than either one by itself.
IMPLICATIONS FOR PREPAREDNESS, AND FUTURE WORK
The Omicron wave of SARS-CoV-2 caused many more cases and deaths than the Delta wave; even by the end of February, the daily death toll of Omicron-driven COVID-19 was greater than total deaths caused by Hurricane Katrina. This burden fell unequally on society, with Americans over 65 representing almost 80% of the deaths, and with significant racial disparities. Results from TRACE suggest many of these cases and deaths were avoidable.
At a time when policy focus and public attention have largely shifted away from COVID, the results above from TRACE also highlight the potential importance of investments now—in booster vaccine uptake and distribution, in testing capacity, in availability of high-quality masks—to prepare for a potential next variant or wave of the virus. Quantifying the potential impact of differing investments can help policymakers make more informed decisions as they weigh the costs and benefits of alternative approaches in future waves.
Finally, both the analysis above and our previous work with TRACE underscore the contributions that policy simulations can make to finding robust and practical policy solutions if they are rooted in models that are spatially and demographically detailed, account for individual behaviors, and manage the uncertainty inherent with fast-moving emerging pathogens.