On November 13, 2022, the Group of 20 (G-20) hosted the official launch of the Pandemic Fund, the new World Bank Financial Intermediary Fund to promote pandemic preparedness and response (PPR). At that event Priya Basu, the executive head of the Pandemic Fund Secretariat at the World Bank, suggested that the fund had only received $400 million of the $1.4 billion pledged by donors (well short of the estimated $10.5 billon that was claimed to be required). Moreover, when questioned about whether substantial new moneys would come into the fund or be diverted from existing aid budgets, Basu stated that “this isn’t just sort of shifting money from one port to another. This is new money.”
However, analysis of new official development assistance (ODA) and national level resource management data reveal some worrying trends that could temper this optimism. These trends suggest that not only did ODA peak during COVID-19, but that resources were reallocated to COVID-19 and PPR activities at the global and national level. Furthermore, there is evidence that these shifts are exacerbating existing health vulnerabilities and weakening overall global health. If these trends continue, then there will be considerable impacts on global health as well as global PPR policies and the Pandemic Fund’s ability to finance them.
Official Development Assistance has peaked and shifted
In May 2022, the Development Assistance Committee of the Organization for Economic Cooperation and Development (OECD DAC) released its annual data on ODA for health. Data are now available for 2020, the year COVID-19 was declared a pandemic. To allow tracking ODA for COVID-19 control, the OECD DAC introduced a new code for reporting COVID-19 ODA.
The data show that in 2020, official donors disbursed $29.1 billion in health ODA, a substantial increase of 31 percent (or $6.9 billion) compared to the previous year (all data reported in constant 2020 prices). Thus in 2020, health ODA reached its highest-ever level. Private flows to health also increased by 21.6 percent, from $4.0 billion to $4.9 billion (Figure 1).
Figure 1. Trends in ODA Disbursements for Health and Private Flows for Health
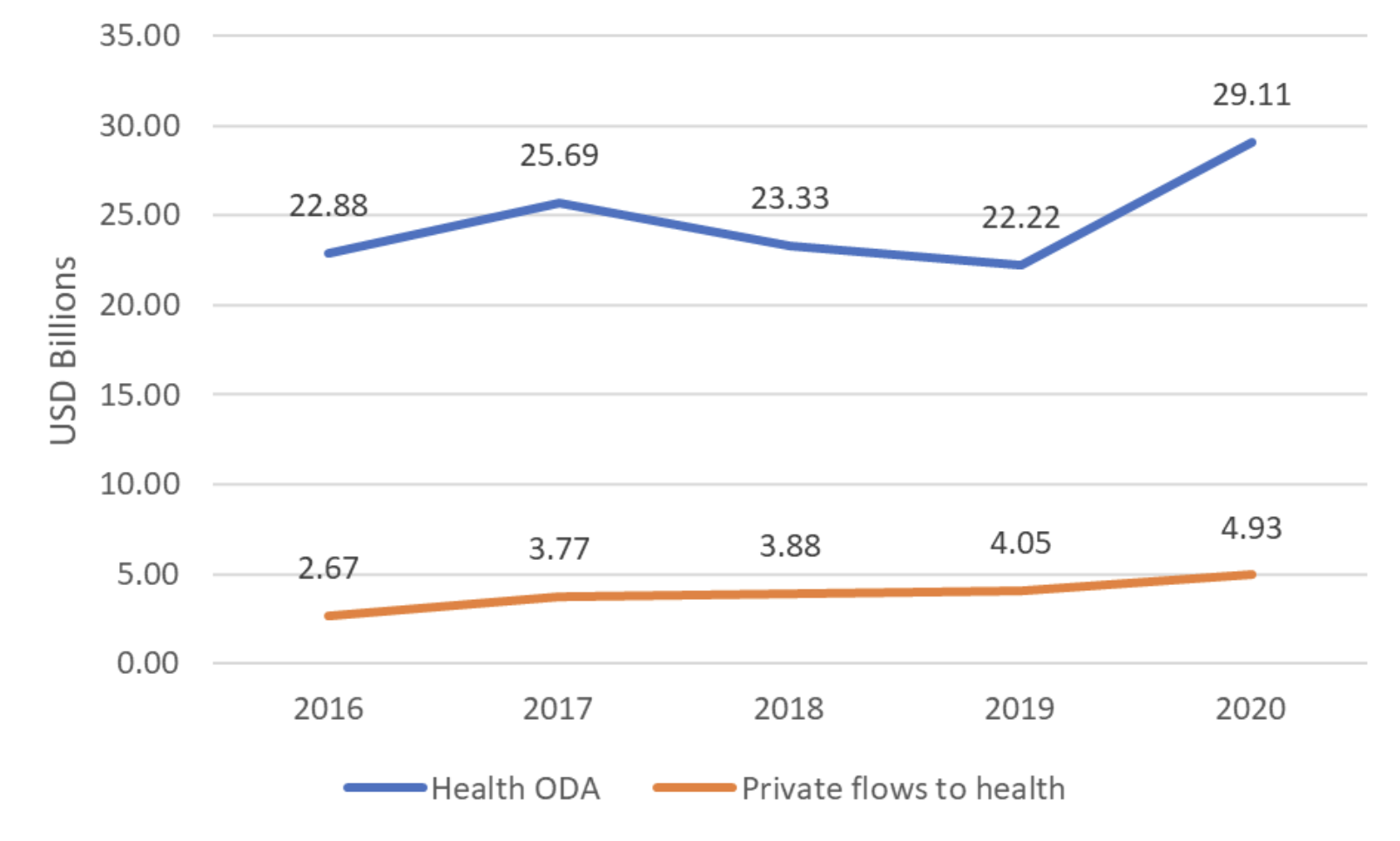
Source: OECD DAC CRS. Gross disbursements, constant 2020 USD prices
Donors disbursed a total of $4.4 billion in response to the COVID-19 pandemic in 2020. A substantial share (63.9 percent) of the increase in health ODA results from donor funding for COVID-19 control. In addition, ODA for infectious disease control grew from $2.3 billion in 2019 to $3.1 billion in 2020. Much of this increase can be attributed to aid activities for pandemic preparedness and response, including for the surveillance, research, and the development of COVID-19 vaccines.
However, the data also reveal areas of concern. Even before the COVID-19 pandemic, most low- and middle-income countries (LMICs) were not on track to achieve Sustainable Development Goal 3 (“Ensure healthy lives and promote well-being for all at all ages”) by 2030. Delivering on SDG target 3.8—achieving universal health coverage (UHC) by 2030—was always ambitious but looks weakened by post COVID-19 ODA. For example, ODA for basic health care fell from $3.4 billion in 2019 to $2.3 billion in 2020, a drop of 34.5 percent. ODA for basic nutrition declined by 10.1 percent. When paired with concerns about donor fatigue in the face of growing global problems (climate, Ukraine, food security, etc.), the outlook for reduced ODA spending and/or diversions of existing funds looks elevated.
Resource shifting and its effect on global health
Beyond the ODA data, there is further evidence that the pandemic has exacerbated UHC vulnerabilities via diversions within national health budgets of LMICs. Particularly from areas such as malaria, tuberculosis, and HIV to COVID-19 and other PPR related activities. Moreover, a study on Ghana found that the COVID-19 pandemic will have an adverse effect on the health financing system in Ghana, including the expected reallocation of government funding for the health sector into COVID-19 related priorities.
Further evidence shows that COVID-19 resource reallocations are reversing progress on health outcomes. For example, evidence suggests broader secondary effects on health systems and outcomes due to COVID-19 takes prioritization away from other health concerns, particularly related to malaria, tuberculosis, sexual and reproductive health and HIV, noncommunicable diseases, and neglected tropical diseases. The World Health Organization reported that 43 countries (including 13 countries with high tuberculosis burden) used GeneXpert machines for COVID-19 testing instead of diagnostic testing for tuberculosis. In addition, 85 countries reported the reassignment of staff in tuberculosis to COVID-19 related duties, while 52 countries confirmed reallocation of tuberculosis budgets to COVID-19 activities. There is also considerable evidence that medical personnel are being reassigned from other health subsystems to COVID-19 related activities. In the case of Indonesia, the diversion of human resources to pandemic response efforts disrupted polio immunization services, putting the country’s polio-free status at risk.
The prospects do not look good—for the Pandemic Fund or global health
There is good reason to believe that a focus on COVID-19 and PPR is pulling resources from UHC with wider health outcome effects. This raises concern that diminished ODA, alongside budget reallocations for increased PPR activity, will increase burdens on already strained health systems while reducing funds available for new initiatives (opportunity costs). There are also signs that global health donors may further reduce their health aid, falling back into a common pattern in global health financing—the “cycle of panic and neglect.” This condition will exacerbate vulnerabilities and health outcomes. Moreover, this will undermine the credibility and sustainability of the Pandemic Fund as existing money is diverted while new money remains scant.
This underscores the need for sustainable long-term funding not only to be well prepared for the next outbreak, but also to support health system strengthening and population health. As the COVID-19 pandemic showed, it is much costlier to respond amid a crisis than to properly invest in global health, including in strong and resilient health systems.
Related Content



Authors





The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).



Commentary
Global health financing after COVID-19 and the new Pandemic Fund
December 7, 2022