
Introduction
Recent high-profile litigation and settlements among states and local governments with drug companies have highlighted the costs of the opioid epidemic on communities. The dollar amounts discussed in some of these cases have been huge. For example, Purdue Pharma and Mallinckrodt agreed to a national settlements of about $10 billion and $1.6 billion, respectively, and a judge in Oklahoma recently awarded a settlement of $465 million in a suit brought against Johnson & Johnson. While these figures are notable, the costs of the opioid epidemic are likely much higher when considering indirect harm to communities and not just the direct costs associated with abatement. The opioid epidemic is a widespread societal problem, and we are only starting to understand the far-reaching consequences that will be borne by individuals and communities.
In this report, we introduce one of the unexplored effects of the opioid crisis, the link between the opioid epidemic and the education outcomes of children in hard-hit areas. Children, of course, are not immune to the effects of what may happen in their homes and communities, and there is ample evidence that negative home or community factors can be associated with lost learning opportunities. One example is that children exposed to higher levels of neighborhood violence have worse education outcomes than children who are less exposed. In a similar vein, childhood exposure to the ravages of the opioid epidemic may result in worse education outcomes.
“The opioid epidemic is a widespread societal problem, and we are only starting to understand the far-reaching consequences that will be borne by individuals and communities.”
Education can be a pathway to economic and social mobility, especially for children from disadvantaged backgrounds. The collateral consequences associated with the opioid epidemic—family members who suffer from substance-use disorder, parents lost to opioid overdose, diverted community resources, and the fraying of neighborhood social connections—have the potential to negatively impact the educational outcomes of children. This may especially be the case for children who grow up in communities hardest hit by the epidemic, such as the Appalachian belt, impoverished rural communities, and the industrial Midwest, potentially exacerbating already existing educational achievement gaps and thus future economic opportunity.
Background on the opioid epidemic
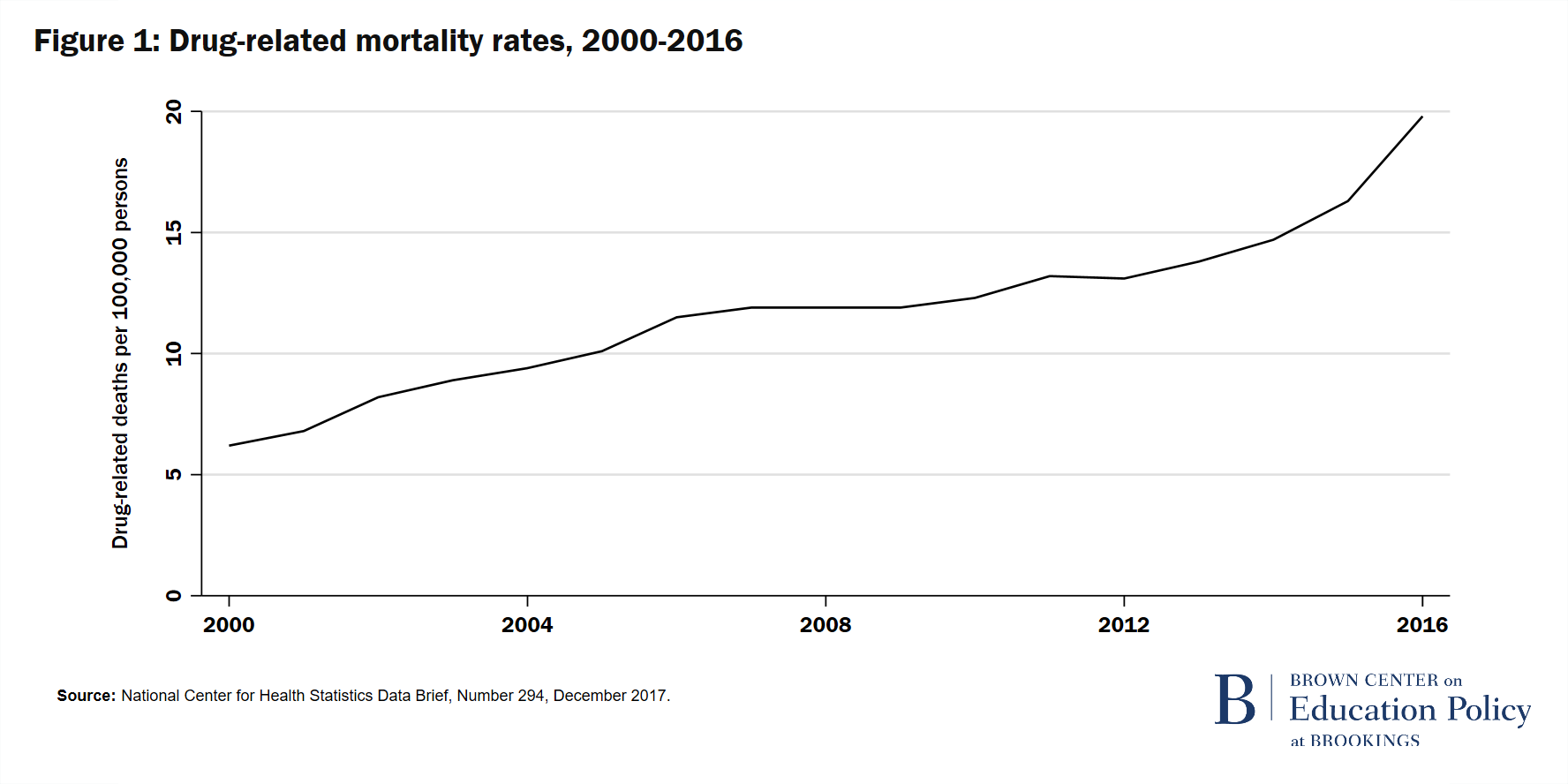
The opioid epidemic is now widely recognized as one of the most important public health issues of our time. In October 2017, Eric Hargan, the acting secretary of the Department of Health and Human Services, declared the “opioid crisis” a nationwide public health emergency, a statement owing at least partly to a dramatic increase in prescription opioid overdose deaths. Opioids are estimated to account for about 70% of drug-related mortality in recent years, and it is the primary driver of variation in these drug-related deaths, according to the Centers for Disease Control and Prevention (CDC). We display age-adjusted drug overdose mortality trends from 1999-2016 in Figure 1. Over this time period, the rate of drug-related mortality grew 225% in the U.S.1 Of course, in addition to opioid-related fatalities, there are other potential negative effects of opioid use, including nonfatal overdose emergencies that lead to hospitalization and ongoing addiction with all of the associated negative societal spillovers. Moreover, opioid abuse can co-occur with other substance-use disorders, depression, and other physical and psychological ailments.
Our reading of the literature is that research on the societal effects of the opioid epidemic, as opposed to the direct effects on individuals with opioid-use disorder, is just emerging. We know of only a few studies that look at these “spillover” effects of the epidemic. For example, in a 2017 Brookings Paper on Economic Activity, Alan Krueger related the ramp up of the opioid epidemic to the observed reduction in male labor-force participation. Moreover, studies, such as those described in research briefs from the U.S. Department of Health and Human Services, linked increased rates of child protective services reports, substantiated reports, and placement of children in foster care to increases in drug overdose deaths and drug-related hospitalizations. Our work contributes to this less-established line of research by examining the effects of the opioid epidemic on a critical societal question—how exposure to the ravages of the epidemic may harm the education outcomes of children who live in communities hard hit by the opioid crisis.
Children, education, and opioids
We are aware of no research directly linking the ravages of the opioid epidemic to the educational outcomes of children in affected areas. Generally, there are two channels through which adverse public health issues like the opioid crisis could ultimately affect education outcomes. The first is a direct linkage via opioid substance-use disorder at the individual level. While we expect the negative effects of direct use to be more prevalent among older youth and young adults (and thus more likely to impact outcomes at a secondary or tertiary education level), babies can be exposed neonatally and potentially suffer subsequent harm. The second channel is a less-direct linkage that could affect the education outcomes of younger children who live in families and/or communities that are struggling with the epidemic. At this point, our work is primarily focused on this second channel and on younger children as we discuss below.
In conceptualizing the pathway linking a young person’s exposure to the opioid epidemic to education outcomes, we draw upon work that models how a given neighborhood context can impact the education outcomes of a child. The neighborhood context under consideration is the opioid epidemic in the community, and the route through which the epidemic can impact a child’s education is via the interaction between the child’s level of exposure to the epidemic and the child’s vulnerability to any given level of exposure.
Related Content



Variation in exposure across children can arise from different sources, experiences, and life situations. For example, a child who lives in a household with an addicted parent may face a traumatic home life, maltreatment, or family separation, all consequences of the child’s direct exposure to the epidemic via their struggling parent. Or, a child could be less directly exposed through, for example, routine exposure to news media reporting of opioid-related deaths and arrests, or via emergency-response incidents in the community. A child could also experience some level of exposure to the epidemic via the opioid-related exposures of other children in their peer group or classroom. The point is that childhood exposure to the opioid epidemic can range from the personal and traumatic to the less direct but potentially pervasive. And, the probability of exposure for any child is greater in communities where the epidemic is more severe and intense.
Framing the problem as beginning with a child’s exposure to the opioid epidemic draws on a well-established literature on the effects of childhood exposure to environmental stressors in general. Traumatic or prolonged exposure to a wide range of stressors can lead to toxic stress response, which in turn is causally related to changes in the architecture of a child’s developing brain, changes in brain architecture that can affect learning. Moreover, a body of literature relevant to our study links exposure to violence and trauma in a community to decreased academic achievement.
Moderating the effects of exposure is the vulnerability of the child to the adverse effects of the epidemic, given their level of exposure. We consider a child’s vulnerability to be a function of family, school, and community supports. For example, a family with relatively more resources might have more ability to insure their children against negative exposure through counseling, either familial or professional. Similarly, at a community level, if it is the case that suburban/urban schools or communities have more robust student support systems in place than do rural schools or communities, then we might expect to see a more pronounced and negative effect of the epidemic on education outcomes in rural areas even with the same levels of epidemic exposure for a given child. Conceptually, less access to support would leave children more vulnerable than would be the case for equally exposed peers with greater access to support, all else equal.
The link between opioids and educational outcomes
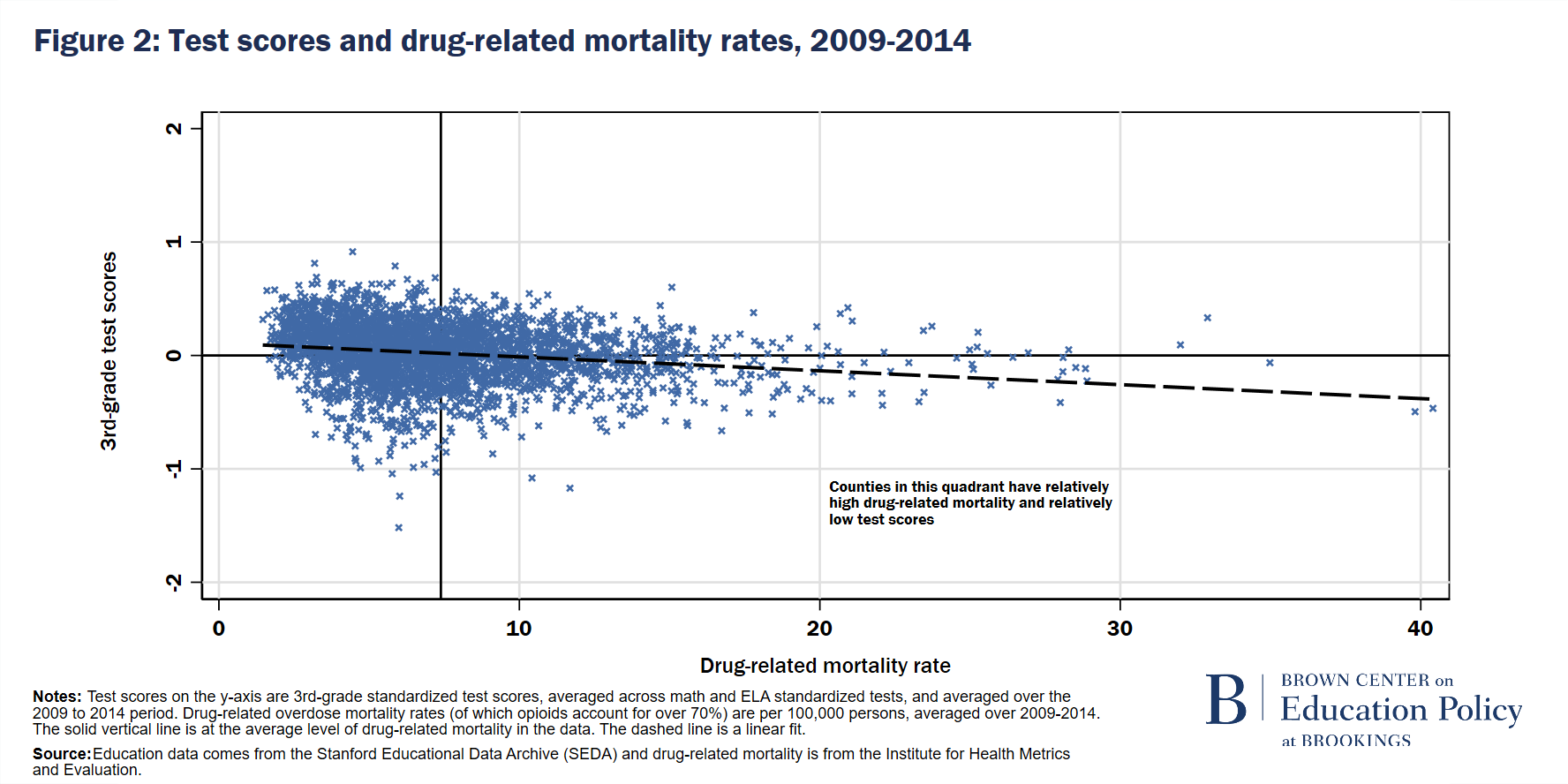
We display a scatter plot of the unconditional relationship between test scores (on the y-axis) and drug-related overdose mortality rates (on the x-axis) in Figure 2 below. The dashed line is a linear fit, which indicates a negative relationship between test scores and drug-related mortality, on average. The solid horizontal and vertical lines are the average level of test scores and drug-related mortality rates in our data. Counties in the upper left quadrant have test scores and drug-related mortality rates that are both relatively low. Counties in the bottom right quadrant of the plot, alternatively, have both high drug-related mortality rates and low educational outcomes for students, which suggests that students in these counties may be at greatest risk for being negatively affected by the opioid epidemic. Conspicuously, there are numerous counties with relatively very high drug-related mortality rates (the markers on the far right of the graph), and most, but not all, of these counties have relatively low test scores. It’s also worth noting that while there is an evident negative relationship between test scores and drug-related mortality on average, there are many counties that have relatively low test scores and relatively low mortality rates (lower left quadrant) or relatively high test scores and relatively high mortality rates (upper right quadrant). Obviously, the opioid epidemic is not the only factor that influences students’ educational performance, but it also suggests that a given level of the opioid epidemic may differentially affect distinct communities.
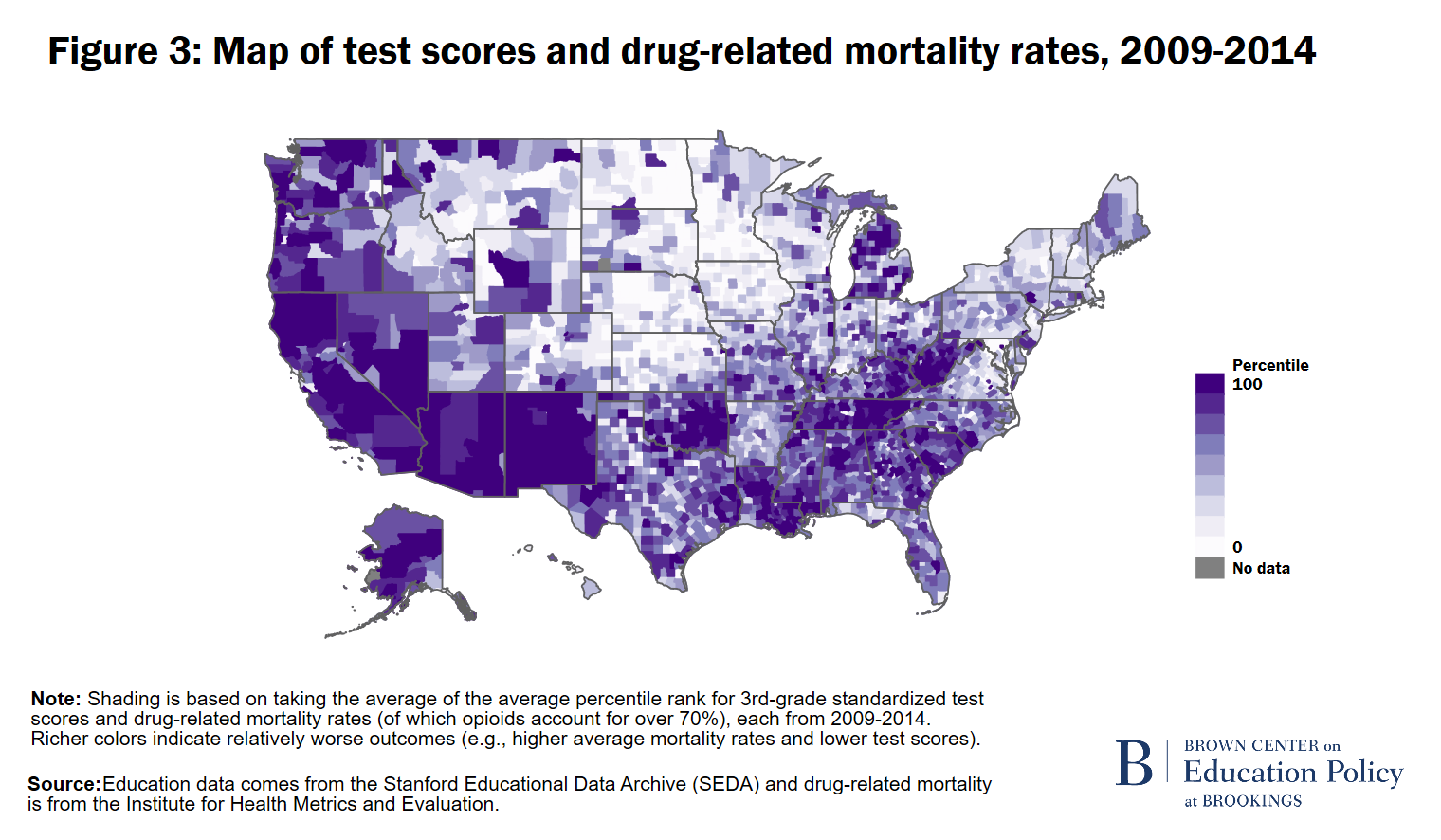
Neither educational performance nor opioid abuse is evenly distributed geographically. In Figure 3 below, we display the geographical intersection of poor educational outcomes and drug-related mortality rates.2 The richer shading in these graphs represent particularly troubling opioid—education “hot spots.” These are counties with relatively high levels of drug-related mortality rates and relatively low test score performance, akin to the counties in the lower right quadrant of Figure 2. The Appalachian belt is notable–this runs from northern Alabama and Georgia, through eastern Tennessee, Kentucky, western South Carolina and North Carolina, and up into West Virginia, and parts of Ohio, Virginia, and Pennsylvania. Similarly, the Southwest and West stand out, with troubling hot spots throughout New Mexico, Arizona, Nevada, and California.
The map, along with the scatterplot, indicate that there are substantial areas of the nation where test scores are low and drug-related deaths are high. We dig further into these relationships links by estimating the linkage between test scores and drug-related mortality while controlling for observed school district and county characteristics, including per-pupil expenditures, county demographics, poverty rates, and unemployment rates.3 While these estimates offer suggestive evidence that exposure to the opioid epidemic and its collateral consequences negatively impacts the learning of children, they do not establish the causal connection that could better inform policy initiatives. This is the first of several studies in which we explore this topic, and our further studies will get us closer to credible evidence of the causal link.
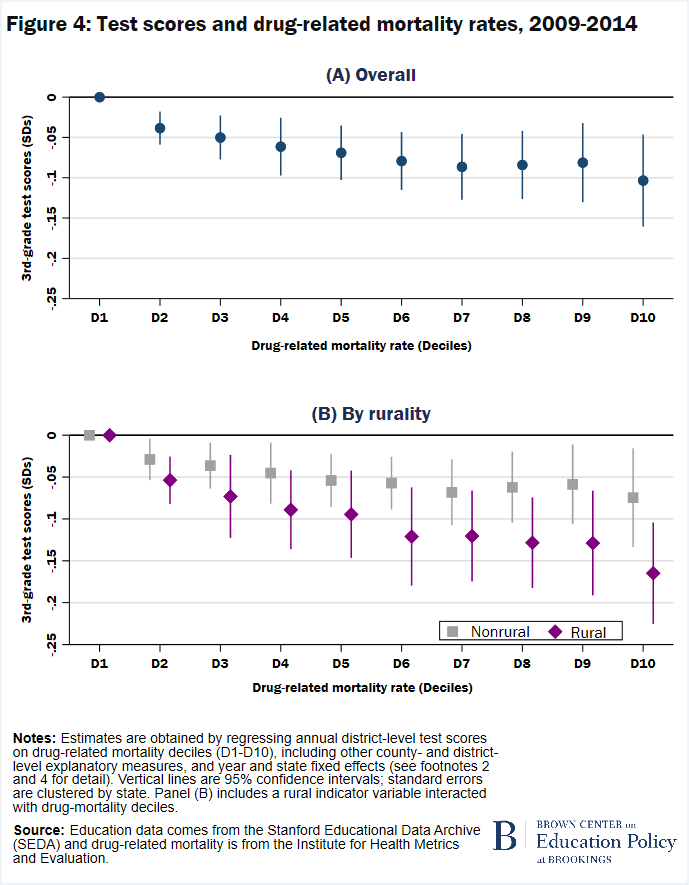
In Figure 4 below, we plot the results from these estimates by decile of drug-related mortality rate.4 There is a downward trend among the parameter estimates, indicating that test scores are progressively lower where mortality rates are higher. These estimates suggest that counties in the highest decile (10th) of drug-related mortality have 3rd-grade test scores that are about a tenth of a standard deviation lower than test scores in the lowest decile (1st) of drug-related mortality. As displayed here, and in Figure 2, there is a long right tail in the distribution of mortality rates, such that the notable jump in drug-related mortality from the 9th to 10th decile could help explain the relatively large coefficient for the 10th decile in some of the figures.
To be clear, in this report we are presenting and discussing conditional correlations; that is, correlations between the opioid crisis and education that have accounted for some, but potentially not all, confounding factors. As mentioned earlier, we anticipate that our future work will allow us to zero in on the causal effect between the opioid crisis and education outcomes. Further work is also needed to understand the types of support that may be effective at reducing students’ vulnerability to the epidemic, and at what level (e.g., familial, school, or community) these supports should be employed.
“[T]he role of the opioid epidemic in affecting educational outcomes may be especially concerning in rural areas.”
Next, we examine how the link between test scores and drug-related mortality differs among rural versus nonrural counties, with rural counties designated as those with greater than 75% of their population in a rural area. Building on the results displayed in panel (A), the estimates in panel (B) allow for the epidemic-test score relationship to differ between rural and nonrural counties. We see that, among both rural and nonrural counties, test scores are lower in counties with higher drug-related mortality. However, the estimated test scores for rural counties are always lower than those of nonrural counties in the same decile of mortality rates (though not always statistically different), even when accounting for local economic and educational conditions. Moreover, panel (B) indicates that the rural-nonrural gap appears to grow as mortality levels increase. These results offer suggestive evidence that the role of the opioid epidemic in affecting educational outcomes may be especially concerning in rural areas, consistent with our expectations about community vulnerability described above. The magnitude of that difference between locales is noteworthy: Rural counties in the highest decile (10th) of drug-related mortality have 3rd-grade test scores that are almost two-tenths of a standard deviation lower than rural counties in the lowest decile (1st). This is about twice as large as the analogous comparison among nonrural counties.
It is likely that students in a community are affected differentially by the opioid epidemic. To investigate this, we next consider in Figure 5 how opioids relate to achievement gaps between students who are and are not considered economically disadvantaged (ECD).5 If ECD students have fewer familial resources to insure their children against exposure to the opioid epidemic, as suggested in our conceptual framework, we may see nonECD-ECD gaps widen as exposure to the epidemic increases. Similar to Figure 4, we set the coefficient for the first decile (i.e., the counties with mortality rates in the lowest 10%) to be equal to zero, such that each marker represents, at that decile in mortality rate, the gap in scores between less and more economically disadvantaged students relative to that gap in the first decile of mortality.
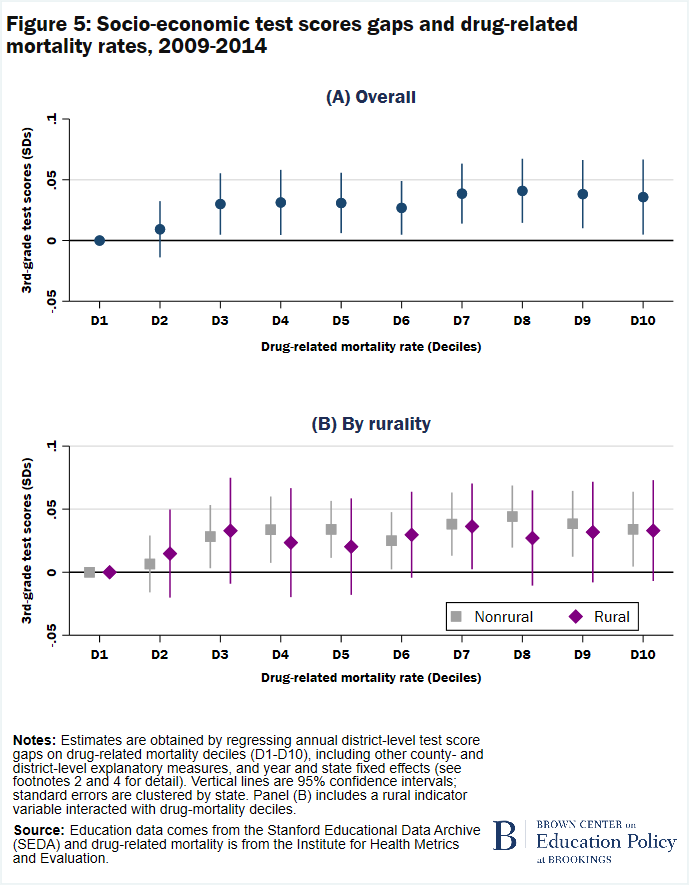
As seen in the top panel, the nonECD-ECD gap is larger in the 3rd to 10th deciles, as compared to the 1st decile, though the point estimates are only mildly increasing over this range. In panel (B), we display heterogeneity in the link between nonECD-ECD test score gaps and drug-related mortality among rural versus nonrural counties, again with rural counties designated as those with greater than 75% of their population in a rural area. Here, we see relationships that are quite similar among rural and nonrural counties. Taken together, results displayed in Figure 5 do not reveal a strong pattern to suggest that ECD students, at least based on the definition available in the data used here, have lower test scores on average when exposed to similar levels of the opioid epidemic as compared to their nonECD peers within the same county—a preliminary finding that deserves further inquiry.
Discussion
To our knowledge this is the first use of national data to examine the relationship between the nation’s opioid epidemic and the education outcomes of our children. To this point, much of the opioid epidemic research has been focused on those most directly impacted by the epidemic: individuals with opioid substance-use disorder.
Our research agenda focus has been less proximate as we ask: What is the effect on children’s learning of being embedded in a community where the opioid epidemic has taken hold? In this case, we have focused on the collateral damage that impacts children and potentially manifests in measurably reduced learning outcomes. Our evidence, while only correlational in this report, suggests a need to be aware of the potentially negative effects of the opioid epidemic on the education outcomes of children. For brevity, this report examined only one education outcome: 3rd-grade test scores. However, it is certainly possible that detrimental educational effects of exposure to the opioid epidemic vary depending on the age and developmental stage of the exposed individual. Moreover, exposure to the epidemic is likely to impact important education outcomes other than test scores, such as attendance, probability of school disciplinary action, graduation, or college enrollment. We are exploring a broader set of outcomes in forthcoming work.
“Our evidence, while only correlational in this report, suggests a need to be aware of the potentially negative effects of the opioid epidemic on the education outcomes of children.”
With those caveats in mind, graphically and with conditional estimates we have shown strong correlations between counties that have high drug-related mortality rates and counties with worse education outcomes among young children. From a visual standpoint, it is also clear that there are “hot spots” of high drug-related mortality and low test scores, and the negative education-epidemic relationship is even larger in rural areas, pointing to the importance of the rural-nonrural divide. While more work is needed to understand the specific challenges that rural counties face in coping with the ravages of the epidemic, we hypothesize that school or community support mechanisms can play an important role in bolstering the academic performance among the most vulnerable children.
It is beyond the scope of this report to recommend specific support mechanisms in how states, school districts, and schools should respond to the problem at hand, and we are cautious to avoid strong recommendations since there is limited evidence on the efficacy of current attempted solutions. We view this report instead as a first step in raising awareness of the potential collateral damage of the opioid epidemic. Nonetheless, we can generally consider opioid-related factors that might affect the academic performance of children to highlight possible points of intervention.
Our previously described conceptual framework allows the opioid epidemic to negatively affect children through the interaction of their exposure and their vulnerability given exposure. It would be difficult for schools to address a child’s direct exposure to the epidemic as a result of what may be happening at home or in the community that results in childhood exposure to the epidemic. However, schools have a role to play in reducing the vulnerability of their students to the aftermath of these experiences or incidents. For example, children may be better positioned to deal with trauma if they have greater access to school counselors and support personnel. The emergence of the “trauma-sensitive school” model is one promising approach to providing school-based supports aimed at helping students cope with trauma. Schools could also reduce vulnerability by coordinating with other community services. For example, the Handle with Care program in Charleston, West Virginia, and replicated elsewhere works to coordinate emergency responders and local school officials so that if, for example, emergency personnel respond, for any reason, to an address where a minor child is present, school officials will be notified before the start of the next school day. Thus, school personnel will be more aware that a child had or witnessed a potentially traumatic experience and will be “handled with care” as per the training of school personnel that is a part of the program.
“Many of the communities where children have the highest exposure to the opioid crisis also have relatively low revenue levels, potentially limiting the assistance and programs schools can offer to reduce children’s vulnerability.”
A challenge associated with building such supports to reduce children’s vulnerability to the opioid epidemic is that school and community resources are not equally distributed geographically. The opioid crisis is often particularly acute in areas that are also experiencing other types of hardship, such as challenging economic and job-market conditions. These conditions can tax available community and health supports and can also affect resources available to schools. A relevant measure of resource constraints relates to the amount of revenue a school or district brings in, as this represents financial capital that could be potentially deployed to fund support for affected children.6 Examining school district revenue reveals a troubling pattern: Many of the communities where children have the highest exposure to the opioid crisis also have relatively low revenue levels, potentially limiting the assistance and programs schools can offer to reduce children’s vulnerability.
This report presents a new and potentially troubling side of the nation’s opioid epidemic, namely, the adverse effects this scourge may be having on learning potential of our children. This report is a first step in examining the connections between the opioid epidemic and education outcomes, and these findings demonstrate the need for both further research that interrogates how this relationship works and the role resources may play in mitigating the negative impact of the epidemic on the education of the nation’s children.
The Brookings Institution is a nonprofit organization devoted to independent research and policy solutions. Its mission is to conduct high-quality, independent research and, based on that research, to provide innovative, practical recommendations for policymakers and the public. The conclusions and recommendations of any Brookings publication are solely those of its author(s), and do not reflect the views of the Institution, its management, or its other scholars.
The findings, interpretations, and conclusions in this report are not influenced by any donation. Brookings recognizes that the value it provides is in its absolute commitment to quality, independence, and impact. Activities supported by its donors reflect this commitment.
Authors

-
Footnotes
- Opioid overdose trends are often characterized in waves: The first wave involving prescription opioids started in the 1990s, the second wave due to heroin starting around 2010, and the third wave involving synthetic opioids, notably fentanyl, ramped up around 2013.
- Data sources used in this report are as follows: The measure of opioid we use here is drug-related mortality data from the Institute for Health Metrics and Evaluation (IHME, http://www.healthdata.org/) which is based on death record data from the CDC. Opioids are estimated to account for about 70% of drug-related mortality in recent years and is the primary driver of variation in drug-related deaths over the time period (CDC, nd). As a measure of educational outcomes in this report, we use 3rd-grade math and reading test scores from the Stanford Educational Data Archive (SEDA).
- Specifically, we estimate: where, Y is educational outcome for county i in state s and year t; M is a vector of indicators for mortality rate deciles drug-related mortality rate in the county averaged over the prior nine years; E is a vector of district-level education measures (% Black/African American in 3rd grade; % Hispanic/Latino in 3rd Grade; % English language learners; % special education; # of schools; # of charter schools; pupil-teacher ratio; expenditures per pupil); C is a vector of county-level measures, all from 2010 (% with a bachelor’s degree or higher; % foreign born; median household income; % of household in poverty; % single parents; % non-white race/ethnicity; population density; total population; total area [in millions of square miles]; % rural population); U is a vector of county-level economic measures (unemployment rate; annualized job growth 2004-2013; job density in 2013); dt and ds are year and state fixed effects; and standard errors are clustered by state. In the estimates by rurality, we estimate the following, where R is an indicator for a rural county (defined here as having ≥75% of the population in a rural area):
- In Figures 4 and 5, D1-D10 represent the first to 10th decile in drug-related deaths per 100,000 persons, averaged for the nine prior years. Standardized test scored are averaged across math and ELA standardized tests in 3rd grade. We set the coefficient for the first decile (i.e., the counties with mortality rates in the lowest 10%) to be equal to zero, such that each marker represents how much lower the test scores (Figure 4) or test score gaps (Figure 5) are in counties with drug-related mortality rates in that decile, relative to the first decile.
- We use the measure of economic disadvantage available in SEDA, which is based on states’ definitions reported to the EDFacts data collection coordinated by the U.S. Department of Education.
- We examined data from the Local Education Agency (School District) Finance Survey (F-33) Data from the U.S. Department of Education, National Center for Education Statistics for 2014.
The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).


