Editor’s note: This blog was written as part of the Center for Health Policy’s Global Accountable Care in Action series that features three long-form case studies focusing on care delivery innovations in Spain, Mexico and India.
View the entire series here
.
Approximately 60 percent of all deaths in India result from chronic or non-communicable diseases (NCDs). Over 8 percent of adults, or approximately 67 million people, in India have diabetes. The state of Tamil Nadu in southeast India has some of the highest rates of hypertension, hyperlipidemia, and diabetes in the country. At the same time, with public spending equal to only 1.3 percent of GDP coupled with a further 20 percent reduction in 2015, many Indians cannot access quality care in the publicly-funded health care system or afford expensive private health care.
To address these problems, SughaVazhvu Healthcare now offers chronic disease care subscription packages for its rural population, which cost less than $2 USD per month.
How does this relate to the U.S.?
Over 9 percent of the U.S. population has diabetes and effective care management for chronic diseases, such as diabetes or hypertension, requires active patient engagement and team-based coordinated care. The U.S. can learn from diabetes programs that foster frequent care interaction and patient support outside clinical settings for effective engagement. Using a subscription program similar to SughaVazhvu, where patients pay upfront for services, may encourage a stronger commitment from patients since they have more of a financial obligation to stay involved.
What lessons can be learned from the subscription packages in India?
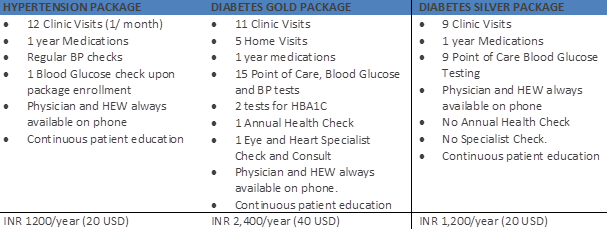
The subscription packages includes all diagnostic, medical, and prescription costs for a defined period of time. The goals of the subscription program also include providing more efficient, team-based care that maintains the condition and prevents complications, such as cardiovascular disease or kidney failure. The SughaVazhvu model also extends care into community settings by expanding the network of community centers and encouraging regular at-home patient visits. In addition, all clinicians and community health workers have access to patient electronic health records. The business model helps drive quality improvement by allowing patients to withdraw from the program if they are not receiving high-valuevaluable services. Figure 1 shows the types of packages SughaVazhvu offers to its patients.
Figure 1:
Chronic Care Package Annual Components
Since 2013, the subscription plan has improved patient satisfaction and increased health care utilization. In addition, since patients pay for a portion of the costs themselves, SughaVazhvu faces pressure to achieve high levels of patient engagement and satisfaction in order to retain payments.
To read more about SughaVazhvu Healthcare and their subscription program, please check out the extended India: Enhancing Care Management for Diabetes Patients in Rural Communities case study that examines the model according to the Global Accountable Care Framework.
The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).



Commentary
What can the U.S. health system learn from India?
April 6, 2015