Medicaid provides health insurance to 79 million low-income Americans and is an important source of health insurance for older Americans, with 16.2 million enrollees ages 45 to 64 and 9.4 million enrollees ages 65 and older in 2021. Medicaid is administered by the states but receives the majority of its funding—70% on average—from the federal government.
The recently passed congressional budget resolution calls for large reductions in spending that would partially offset the costs of a large package of tax cuts, including extending the 2017 Tax Cuts and Jobs Act. The resolution instructs the House Energy and Commerce Committee to recommend changes in programs under its jurisdiction—including Medicaid—that reduce the deficit by $880 billion over 10 years. Because Republican lawmakers and the White House have put Medicare off limits, the Congressional Budget Office has indicated that achieving this target will not be possible without imposing significant cuts to Medicaid.
Reducing federal funding for Medicaid can be done in a variety of ways. We focus here on two specific changes that appear to be under active consideration by congressional Republicans.
The first is reducing the share of costs the federal government pays for the Affordable Care Act (ACA) Medicaid expansion population—90%—to the share that currently applies to other eligibility groups (50—76.9%, depending on the state). This change would specifically impact states that expanded their Medicaid programs to cover nearly all low-income Americans under age 65 under the ACA and could affect state decisions about whether to continue these expansions. In fact, 12 states have enacted so-called “trigger laws,” some of which would automatically end their Medicaid expansion programs were the federal government to lower the matching rate.
The second is introducing work requirements as a condition of Medicaid eligibility. These proposals would involve establishing a set of “community engagement” requirements and a verification process that beneficiaries would have to comply with in order to maintain Medicaid coverage. While some Senate Republicans have expressed opposition to certain types of Medicaid cuts, introducing work requirements in Medicaid has garnered greater support.
In this brief, we discuss the specific pathways to Medicaid eligibility for near-elderly Americans, those age 50 to 64, and analyze the ways these proposals are expected to impact Medicaid beneficiaries in that age group. We find that coverage losses for this group are likely to be large and that these losses would likely reduce their access to and utilization of health care services and would in turn result in compromised management of chronic conditions, greater risk of mortality and morbidity, and increased costs to the Medicare program.
Pathways to Medicaid enrollment for older Americans
The way older Americans qualify for Medicaid differs by age group. To start, we examine rules that apply to adults under age 65, with a specific focus on how eligibility depends on whether or not a person has a disability.
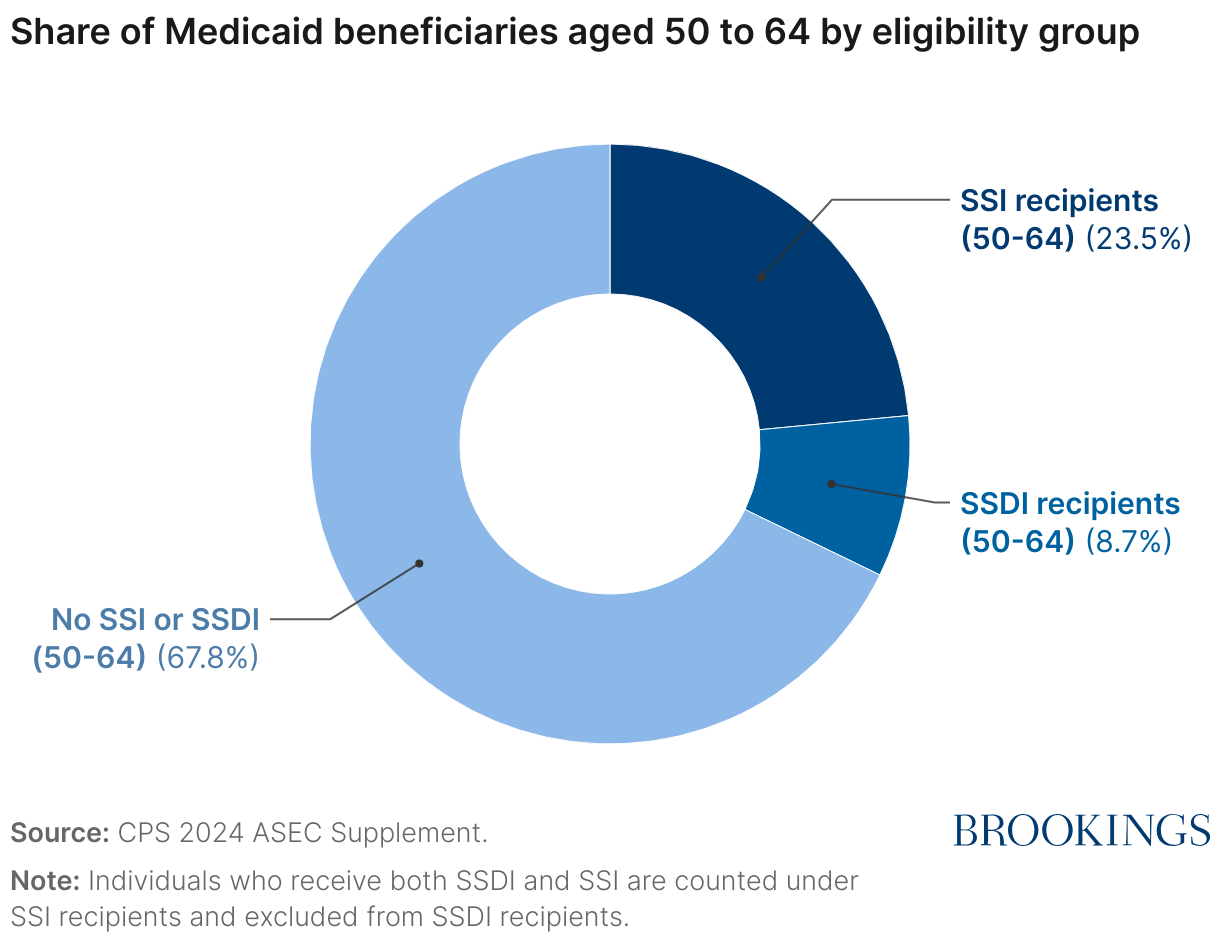
Medicaid enrollees aged 50-64 can be usefully divided into three groups. The first group consists of those receiving Supplemental Security Income (SSI), a program administered by the Social Security Administration that provides monthly benefits to people with limited income and resources with a qualifying disability. Federal law requires states to cover much or all of this group, and, in practice, most states enroll SSI beneficiaries into Medicaid automatically. Approximately a quarter—23.5%—of Medicaid enrollees aged 50 to 64 receive benefits from SSI (compared to 7.6% of Medicaid enrollees aged 19 to 49).
The second group consists of those receiving only Social Security Disability Insurance (SSDI) and account for 8.7% of 50-64 year-old Medicaid beneficiaries.1,2 Most SSDI recipients are eligible to receive health insurance from Medicare. Some SSDI recipients with low incomes also qualify for coverage by Medicaid. For these so-called dually eligible beneficiaries, Medicaid may help pay Medicare premiums or cost-sharing and/or provide coverage for services Medicare does not cover. Additionally, Medicaid can function as the primary insurer for SSDI recipients during the 2-year waiting period for Medicare coverage.
SSDI beneficiaries can qualify for Medicaid in multiple ways. States must offer premium and cost-sharing assistance to low-income Medicare beneficiaries via the so-called Medicare Savings Programs, although participation in these programs is low. Beneficiaries seeking coverage for a broader array of services may qualify either through certain non-SSI eligibility pathways for people with disabilities or solely based on having a low income, as discussed further below.
The remaining share of Medicaid enrollees aged 50 to 64—67.8%—are not receiving SSI or SSDI, although 19.7% of these enrollees still report having at least one disability, albeit not one that has qualified them for SSDI. These enrollees typically qualify for Medicaid based solely on income. While federal law requires states to cover some very low-income parents, which accounts for some coverage in this group, most of these enrollees likely qualify via the state option to expand Medicaid to all low-income adults that was created in the ACA.
Work requirements would likely cause large coverage losses and not increase employment
A federal work requirement would likely directly exclude Medicaid recipients who are also receiving SSI or Medicare. Thus, we focus our analysis on Medicaid recipients age 50 to 64 who did not meet these criteria, a group that we estimate contained 6.1 million people in 2023.
Some past work requirement proposals have not applied to the full 50-64 age range. Notably, the federal work requirement in the Limit, Save, Grow Act passed by the House of Representatives in 2023 would only have applied up through age 55. Nevertheless, we believe it is possible that future proposals would encompass a broader range of ages, so we consider the full 50-64 age range here.
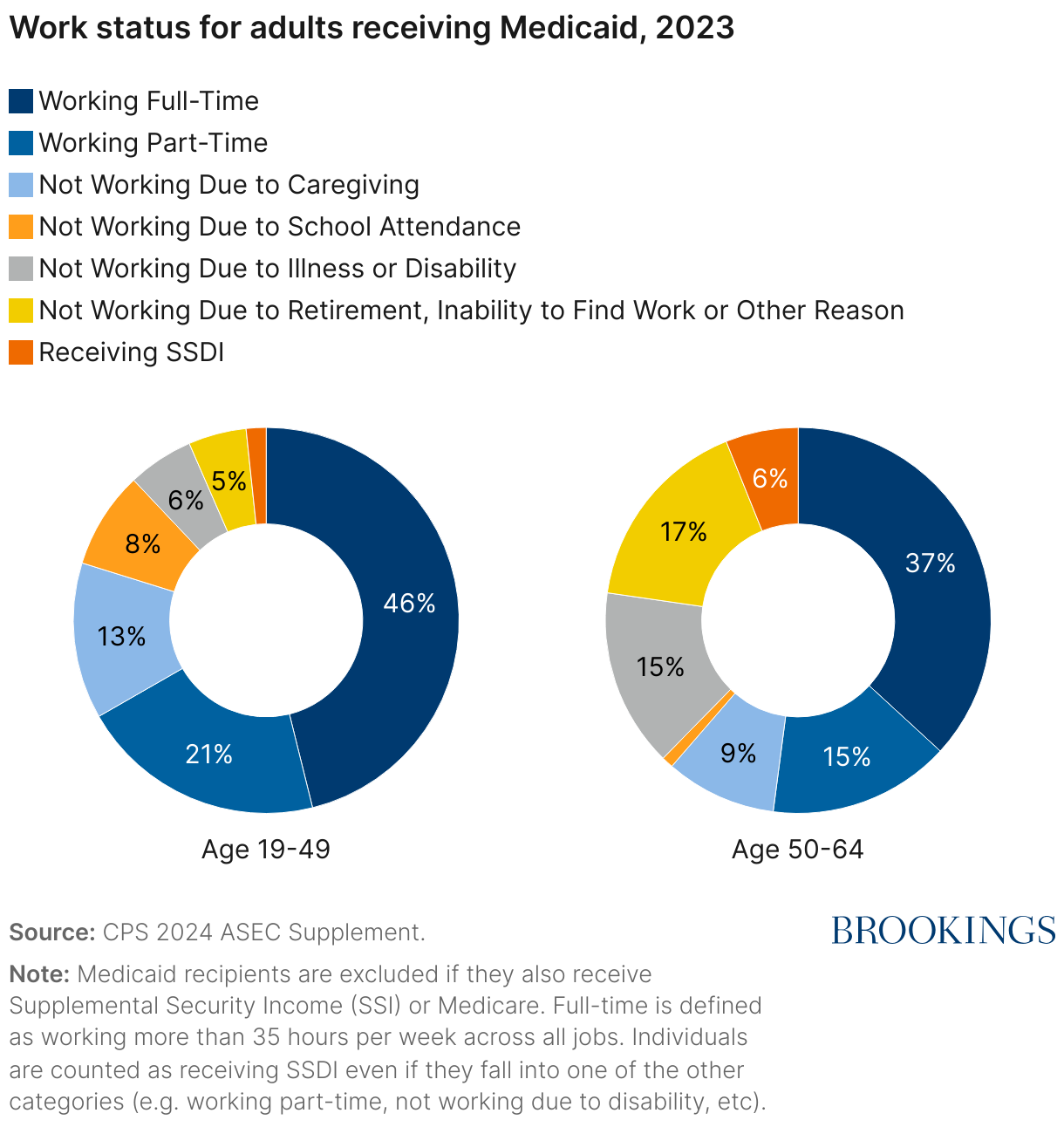
Among Medicaid recipients not receiving SSI or Medicare, 52% of those ages 50 to 64 were employed, compared to 67% of those ages 19 to 49. Within the age 50 to 64 group, 37% worked full time and 15% worked part time, compared to 46% and 21%, respectively, for 19-49 year-olds. The reasons for non-employment varied as well, with the younger group reporting caregiving and school attendance as the most common reasons for not working, while illness or disability was a more common reason among 50-64 year-olds, accounting for almost one in six enrollees in this group potentially subject to work requirements. This is notably much larger than the 6% of the sample receiving SSDI benefits.
Medicaid has traditionally not tied eligibility to employment. However, during the first Trump administration, the Centers for Medicare and Medicaid Services provided an avenue for states to do so via Medicaid waivers.3 From June 2018 through February 2019, Arkansas applied a work requirement to Medicaid beneficiaries ages 19 to 49 and began implementing changes for 30-49 year-old beneficiaries.4 For some enrollees, the state was able to assess compliance with the policy using data it already held, however many enrollees were required to submit periodic reports showing that they were engaged in the required activities or met the criteria for an exemption (e.g., because they were taking care of a family member). Enrollees who were non-compliant for three months were disenrolled from Medicaid.
While the details, implementation, and context of the work requirement in Arkansas may not directly apply to the federal case, evidence from the Arkansas experience can help inform how work requirements may impact outcomes if implemented nationwide. By December 2018, about 24%5 of beneficiaries subject to the requirement were disenrolled. Evaluations found no evidence that this reduction in Medicaid enrollment was accompanied by an increase in other sources of insurance coverage, employment, hours worked, or participation in other qualifying activities. The percentage reduction in coverage was even larger among those with chronic conditions, men, and non-Hispanic whites, and follow up research showed that those who lost coverage experienced significant difficulties in paying off medical debt, cost-related delays in care, and lapses in medication adherence.
These findings are consistent with the evidence from work requirements for the Supplemental Nutrition Assistance Program (SNAP), which showed that work requirements reduced program participation by 53% with no corresponding effects on employment. This body of evidence has led experts to conclude that losses from a nationwide work requirement would be large and significant, with estimates of 4-5 million people losing Medicaid coverage—and this number would be larger if work requirements were to extend beyond age 55. While the Congressional Budget Office (CBO) projected smaller coverage losses in their analysis of the 2023 House bill, their analysis assumed that states would choose to cover these individuals with state funds. Importantly, all of these analyses predict that such requirements would not be accompanied by higher employment rates.
The Arkansas requirement did not apply to the near elderly; however, there are many reasons why imposing work requirements could lead to more significant consequences among 50-64 year-olds. While the higher valuation of health insurance among older Americans might increase the incentive to work in order to keep Medicaid coverage, work capacity among 50-64 year-olds is likely even lower than those who are younger, given that 15% of this group reports not working due to illness or disability compared to 6% among those 19 to 49. There is evidence that those who look for work in this age group experience age discrimination in hiring, limiting employment opportunities among those with work capacity. Finally, the higher prevalence of chronic conditions among 50-64 year-olds combined with the evidence from Arkansas suggests that disenrollment would be proportionally higher among older Americans.
3 million near-elderly Americans could lose health insurance if federal matching is cut
There are about 5 million people6 aged 50 to 64 that are eligible because of the Medicaid expansion who are at risk of losing coverage if federal support for the ACA Medicaid expansion were reduced. The impact of such a proposal turns on the likelihood that most Medicaid expansion states would compensate for the loss of federal funds by scaling back on coverage.
It is likely that a few states, particularly those that extended Medicaid coverage to some adults prior to the ACA like Vermont and Massachusetts, will be willing and able to replace the lost federal funding. Yet we know that 12 states have laws that trigger either reconsideration or dropping of expansion coverage if the matching rates are lowered. Beyond those, the combination of balanced budget requirements, the large share of state budgets currently accounted for by Medicaid, and sluggish growth in state revenues makes it unlikely that most expansion states would continue their commitments to an expanded Medicaid program. Furthermore, prior to the ACA, only 11 states extended Medicaid coverage to parents, and only two states to other adults, with income at or above 138% FPL.
The implications of numerous states retreating from Medicaid expansion are several. Analyses based on the Medicaid expansion experience suggests that elimination of that coverage would leave about 64% to 68% of those currently covered—including about 3.3 million people aged 50 to 64—newly uninsured.
Coverage losses among 50–64 year-olds are particularly harmful
The loss of health insurance coverage among 50–64 year-olds from either imposing work requirements reducing federal support for the Medicaid expansion population is expected to be particularly costly. The lack of insurance means that access to care will decline and with it, regular visits to physicians, prescription drug fills for chronic conditions, and management of those conditions, which are much more prevalent among this age group. This will in turn likely result in poorer clinical outcomes as well as increases in functional impairments.
It is also likely that reductions in coverage among 50–64 year-olds will spill over to higher Medicare spending when they turn 65, leading to higher costs for beneficiaries and taxpayers alike. Notably, there is evidence that the improved coverage from the Medicaid expansion in the 50–64 year-old age group reduced preventable hospitalizations when they became Medicare beneficiaries at age 65.
There is also evidence that Medicaid expansions reduced mortality rates among those newly covered by the program. A review of the literature on health insurance and mortality finds that Medicaid coverage reduces mortality, specifically for older adults in the short-run and children in the long-run. In particular, recent studies of ACA and Massachusetts health reform show that coverage expansions resulted in significant reductions in mortality. One study found a 2.9% reduction in all-cause mortality in Massachusetts following the 2006 coverage expansion. Another study estimated a 3.6% reduction in mortality for adults aged 20 to 64 following the ACA Medicaid expansion. For adults aged 55 to 64, one study estimated a 9.4% decline in mortality attributable to the ACA Medicaid expansion. The result is consistent across a variety of different methodologies and populations. The evidence is clear: Medicaid provides life-saving support for millions of Americans, in particular the 50–64 year-olds that would be especially susceptible to cuts to the program.
Related Content

2025
Authors



-
Footnotes
- We include people receiving both SSI and SSDI in the first group and exclude them from the second group.
- SSDI beneficiaries comprise 2.5% of Medicaid enrollees in the 19-49 age group.
- While 13 states were approved for demonstration programs involving work requirements, many were halted by court orders or were rescinded by the Biden administration in early 2021.
- The requirement was not applied after February 2019 due to a court ruling. The state phased in the requirement over this period, so not all enrollees were subject to the requirement in all months.
- We calculate the disenrollment percentage by dividing the total cases terminated from August 2018 through December 2018 (18,164) by the number of enrollees subject to work requirements in September 2018 (76,222) according to the Arkansas Department of Human Services.
- We estimate the number of people aged 50-64 who are enrolled because of Medicaid expansion my multiplying the number of expansion adults (22.5 million) by the share of expansion adults aged 50 to 64 (23%).
The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).



Commentary
How proposed changes to Medicaid are expected to impact near-elderly Americans
May 8, 2025