
This paper is a collaboration between The Brookings Institution’s Governance Studies program and The John Locke Foundation.

Introduction
A combination of escalating costs, an aging population, and rising chronic health-care conditions that account for 75% of the nation’s health-care costs paint a bleak picture of the current state of American health care.1 In 2018, national health expenditures grew to $3.6 trillion and accounted for 17.7% of GDP.2 Under current laws, national health spending is projected to grow at a rate of 5.5% per year between 2018-2027.3 Time, another cornerstone of cost and quality, is yet another category where American health care falls short; it typically takes two hours to see a doctor for 20 minutes in most communities.4 While the Affordable Care Act (ACA) sought to close the uninsured gap, immediate and affordable access to health care was not always available, especially for certain populations. Among people of color, health disparities have been extensively documented, largely due to pre-existing medical or chronic conditions, including those affecting the more aged in this population.5 Rural communities are also impacted by the lack of proximity to local medical facilities and providers.6
In March 2020, the entire health-care system—from hospitals to medical practitioners to first responders—was further challenged by the rapid and mass spread of the novel coronavirus and its associated disease, COVID-19. Medical institutions and providers were impacted by the lack of personal protective equipment (PPE), insufficient patient testing, and institutional stresses in the care of infected persons. Beyond the U.S., negative health outcomes of COVID-19 have debilitated entire countries from China to Italy and more, bringing devastating mortality rates.
While the search for a global vaccination to cure the disease is in process, the stress on medical providers and hospitals prompted a historic move toward the authorization and adoption of telehealth services. Embroiled in decades-old debates over its effectiveness in providing patient care, telehealth has also faced other obstacles to its adoption and use, including licensure, reimbursement, and eligible services. Yet, in response to the coronavirus outbreak, the Trump administration and the U.S. Department of Health and Human Services (HHS) sweepingly approved the use of telehealth services as part of the Coronavirus Preparedness and Response Supplemental Appropriations Act.7 As part of this newly granted permission, most Medicare payment requirements were waived and recipients were able to access remote care, regardless of where they live. During the pandemic, telehealth services were also charged at the same rate of in-person medical services, or at parity. The move to accelerate the use of telehealth services also included other exemptions, including some HIPAA exceptions for providers when Facetime or Skype was used by doctors to communicate with patients.
Before COVID-19, telehealth initiatives provided a platform to combat the shortcomings of cost, quality, and access ingrained in American health care. The breadth of telehealth services includes remote clinical health care, patient and professional health-related education, public health, and health administration via electronic information and telecommunication technologies.8 Health-care delivery services are also integrating artificial intelligence (AI) systems into the suite of telehealth services, as both doctors and patients move from solely remote patient monitoring for continuous recording of vital signs to real-time alerts from a patient sensor when there is a deteriorating change in condition. Further, AI is assisting in the management of chronic conditions, including diabetes and heart disease, and when patients require care from multiple specialists working at different times and locations. In these instances, existing applications, AI, and other emerging technologies are coordinated under the guise of telemedicine for complex treatments, like virtual assistants to help patients carry out treatment plans by sending reminders to take medications and providing relevant health information.9
“State and federal barriers in the use of telehealth and AI have served as hindrances to the launch of its full capabilities.”
Prior to the coronavirus outbreak, telehealth and integrated AI were somewhat familiar though not common in practice. But the increasing use of technology has not necessarily been embraced by the long-standing rules and regulations governing the full body of the health-care system. Until recently, telehealth use has largely been limited, stifled by the ambiguous and often changing regulations on the reimbursement of doctors and licensure, especially across state lines. State and federal barriers in the use of telehealth and AI have served as hindrances to the launch of its full capabilities, particularly those laws that present a patchwork of accepted and non-eligible costs and services. Given that telehealth now has a critical role in the mitigation of COVID-19, how well will the U.S. take guidance from its rapid adoption and use? More specifically, how can telehealth be more visibly positioned as an important aspect of health-care delivery in a post COVID-19 health-care ecosystem? And, will telehealth practices be continued without the previously applied restrictions of state and federal laws, especially those around service reimbursement or parity agreements?
This paper explores these questions to extrapolate what state and federal policies will need to be adopted to potentially prepare for more ubiquitous adoption and use of telehealth services in an expanded set of use cases than those recorded by law. The authors also explore the application of existing and emerging state parity laws, which could serve as an obstacle to telehealth delivery in the future. Despite their application as a framework for reimbursement of COVID-19 expenses during the current application, the paper will provide guidance on these and other state and federal laws that will run counter to the long-term promotion and patient access of digital technologies, particularly those that aid in the management of primary care, chronic health conditions, and prevention. The paper concludes with a set of policy and pragmatic proposals that combine the recent lessons learned by the health-care community and patients, along with larger issues, including broadband access, that set the stage for future use. These recommendations were compiled after a structured focus group with medical practitioners, associations, and health policymakers working on the matters described in this paper.
The state of the U.S. health-care system
The U.S. is the only developed country in the world without a universal health-care system. Instead, the nation has a hybrid public-private system where individuals get their health insurance from their employer, through a public program such as Medicaid or Medicare, purchase it directly on the market, or do not have health coverage at all. While a detailed description of the entire U.S. health-care system is far beyond the scope of this paper, the context offers the reasons why telehealth initiatives must be available to mitigate the absence of universal access, disparate patient costs, and quality care.
Cost is perhaps the leading concern regarding the health-care system in the U.S. The country not only spends more on a per-capita basis than any other country,10 but also typical prices for normal procedures are often far higher than comparable procedures in other countries.11 Studies have also estimated that roughly 30% of medical spending does not necessarily lead to an increase in the quality of patient care or is wasted.12
“Compared to many other countries, the U.S. lags in terms of health outcomes, despite the massive amount spent and far more advanced facilities.”
Compared to many other countries, the U.S. lags in terms of health outcomes, despite the massive amount spent and far more advanced facilities. According to the latest data available, the U.S. ranks below the average measures of life expectancy and infant mortality among OECD countries.13
Adopted under the former Obama administration, the ACA drastically changed the conversation on health-insurance coverage in the U.S. in 2010. The ACA had three primary goals: create marketplaces for affordable insurance to be purchased, expand the Medicaid program to cover those who make too little to buy health insurance in the market, and to innovate health-care delivery in general to lower the overall rise in annual health-care costs.14 Modeled after a Massachusetts state health-care plan, the ACA attempted to extend coverage to as many people as possible through a regulated, competitive individual market. Over 44 million people were without insurance before the ACA went into full effect in 2013.15 By 2017, the number of uninsured Americans dropped to 28.5 million.16
Outside of the ACA, the most common types of health-insurance coverage for those that are insured include: employer-sponsored plans, non-group individual market plans, Medicaid, and Medicare. According to 2017 data compiled by the Kaiser Family Foundation, roughly half of Americans got their coverage through their employer. Seven percent purchased health insurance directly in the non-group market, 21% of Americans had coverage under Medicaid, 14% of Americans had coverage under Medicare, and 1% had other public insurance.17
In recent years, partisan gridlock at the federal level has made state-level regulation and oversight more attractive alternatives for the health-care sector. For example, Senate Democrats required a supermajority of 60 votes to avoid a filibuster and pass the ACA in 2009.18 Since that time, Republicans in the House of Representatives have made numerous attempts to repeal the law in part or in whole, and court battles have also challenged the legality of various provisions from 2010 to 2017.19 The current White House has even attempted to repeal the ACA as individuals manage the health effects of the coronavirus. In the beginning of the ACA’s rollout, technical difficulties also hampered the rollout of online health-insurance exchanges in 2013.20 Technical malfunctions slowed the roll out, forcing some states to do more around general health-care access and telehealth usage for the under- and un-insured.
This crude summary of the U.S. health-care system will obviously raise additional questions, but it is pertinent to the argument of the paper that new advances in telehealth be available to extend health-care access to more people and improve upon patient outcomes. Moreover, with cost often the highest concern for the millions of uninsured, innovation in the delivery of services may decrease cost while reducing opportunities for waste and duplication of services. As seen during the coronavirus outbreak, appropriate public policies are more likely to drive adoption of telehealth practices, which is why Congress and federal agencies, like the Federal Communications Commission (FCC), must continue to promote remote access in the future.
Definitions of telemedicine, telehealth, and digital health
Telemedicine case studies
In 2016, the Chronic Care Management Program at Frederick Memorial Hospital in Maryland launched a remote patient monitoring telehealth platform to improve care management for patients with chronic conditions who aren’t in home health care. The program has seen great success; cutting ER visits in half, reducing hospitalizations by nearly 90%, and cutting the cost of care by more than 50%.21 Enrolled patients are given a tablet loaded with mHealth software and connected to Bluetooth-enabled digital health devices. Hospital care providers can also collect biometric data and regularly monitor and communicate with patients via various platforms including video, phone, or text. These data-driven platforms enable providers to pre-emptively identify health issues before they become more serious and require emergency care.22
In Philadelphia, the JeffConnect telemedicine platform at Jefferson Health Hospital successfully diverted close to 650 patients away from infamously expensive care settings, such as emergency departments, garnering cost savings ranging from $300 to more than $1,500. The program found that most health concerns could be resolved in a single consultation and that new utilization was infrequent. With each JeffConnect visit at a $49 flat fee, about 16% of the surveyed patients admitted that they would have “done nothing” as an alternative to a telemedicine visit, which suggests an incorporation of a subset of patients into the health-care system who may have not previously participated, serving as a cost preventing measure down the line.23
In a third case study, the state of New Jersey has placed an emphasis on utilizing telehealth platforms to enhance primary, behavioral, and mental health care for children and adolescents. Pediatricians are using telehealth to connect with psychiatrists, alcohol and drug counselors, social workers, and case managers to identify and treat behavioral health issues, substance abuse, and trauma.24
Defining telemedicine and telehealth
Each of these case studies demonstrate that telehealth and telemedicine are used interchangeably in most contexts, but they may not always mean the same thing. Specific definitions are important because an examination of policies and regulations, including state laws, can be useful in understanding differences in provider use and reimbursement, especially in how state rules defines the scope of services for telehealth.25
In 2010, the World Health Organization (WHO) published a global report on telemedicine, which settled on this broad definition of telemedicine after an evaluation of numerous peer-reviewed studies:
“The delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities.”26
The WHO also goes on to differentiate between telemedicine and telehealth by saying the former describes services administered by physicians only, while the latter describes services provided by a wide range of health-care professionals, “such as nurses, pharmacists, and others.” According to the WHO, four elements are specific to telemedicine:
- The practices are used to provide clinical support
- It is intended to overcome geographic barriers by connecting users, not in the same area
- It involves the use of various forms of information and communication technologies (e.g., computers, internet, cell phones)
- Its goal is to improve health outcomes.27
Different from the WHO, the American Telemedicine Association (ATA) views the terms as more compatible. According to their website, “ATA largely views telemedicine and telehealth to be interchangeable terms, encompassing a wide definition of remote healthcare, although telehealth may not always involve clinical care.”28
While ATA’s definition allows for some ambiguity related to the definitions of these related terms, the federal government’s health information technology website defines telehealth and telemedicine quite distinctly. Telehealth is “the use of electronic information and telecommunications technologies to support long-distance clinical health care, patient and professional health-related education, public health and health administration.” Telehealth is different from the more specific definition of telemedicine because “it refers to a broader scope of remote healthcare services than telemedicine. While telemedicine refers specifically to remote clinical services, telehealth can refer to remote non-clinical services, such as provider training, administrative meetings, and continuing medical education, in addition to clinical services.”29
Similarly, an in-depth article in the New England Journal of Medicine also distinguishes between telehealth and telemedicine. Telehealth is described as a broader term referring to “the delivery and facilitation of health and health related services including medical care, provider and patient education, health information services, and self-care via telecommunications and digital communication technologies.”30 The article further defines telemedicine as “the remote diagnosis and treatment of patients by means of telecommunications technology.”
“Discerning the differences between telehealth and telemedicine is critical due to the public policy implications and their imposed guidance on the provision of such services.”
Discerning the differences between telehealth and telemedicine is critical due to the public policy implications and their imposed guidance on the provision of such services. The use of telehealth is more commonly used in this paper as we also recognize the distinctions between the two activities.
The future of digital health
It is important to note that focus group participants also inserted a new definition into the debate around remote patient care—digital health. Digital health refers to the plethora of software applications and consumer-facing hardware, such as Fitbits. It also includes categories such as mobile health, information technology, wearable devices, and personalized medicine.31 As discussed by focus group participants, reframing the discussion away from telehealth and toward digital health broadens the scope and impact of the conversation. The actualization of the goals for digital health also brings together a wide array of stakeholders, including health-care providers, researchers, medical-device firms, and mobile-application developers. Compared to both telehealth and telemedicine services, digital health platforms may offer the next generation of greater access to information and platforms for communication, as well as present patients with more innovative ways to self-monitor their well-being, including via fitness apps, glucose monitors, among other things. The American Medical Association has most recently explored digital technology in health care as an emerging and growing market. Their playbook for digital health implementation offers a repository of best practices and questions for medical providers.32
Despite a leaning toward broader conversations on digital health, the authors have chosen to use the term “telehealth” as a way to describe the broad use of telecommunications for health-related services. That terminology will be used throughout the paper, although it is still acknowledged that the term telemedicine refers to specific uses of telecommunications for clinical treatment and diagnoses.
General barriers to telehealth adoption
Prior to the coronavirus outbreak, several major barriers existed for those who wanted to embrace telehealth alternatives. The list of hurdles expressed by both urban and rural health centers involved cost and reimbursement policies, licensure, equipment issues, incompatible electronic health records, and gaps in rural broadband.33 Below, some of these barriers are outlined before describing, in some detail, the federal and state policies that either support or attempt to bypass these limitations.
Reimbursement
Because federal reimbursement policies are centered on Medicare, they are narrowly construed and have imposed limitations on where telehealth services may take place, both geographically and by facility, and what services are covered. Moreover, each state dictates separate Medicaid policies, creating a patchwork of telehealth laws and regulations across the nation. Over the last few years, states have begun to pass legislation to encourage private payers to reimburse telehealth-delivered services.34
However, telehealth laws have been written in such a way where they may be a parity in coverage services, in payment, or both. While payment parity acts as a strong incentive for more physicians to adopt telemedicine platforms, enforcing equal payment could also undermine telemedicine’s cost-effectiveness.35 Legislative directives have long impacted the delivery of telehealth initiatives, largely because the meaningful adoption of telehealth often rests on statutory language.
“While fully embracing telehealth under existing state and federal policies should be priority, new policies must address evolving concerns related to reimbursement policies and licensing laws.”
While fully embracing telehealth under existing state and federal policies should be priority, new policies must address evolving concerns related to reimbursement policies and licensing laws. Payment models that reward value in the remote delivery of services, rather than paying providers at capped rates (regardless of the service) may encourage providers to utilize telehealth as a service, particularly in a redefined approach.36 Further, streamlining the credentialing process with standard requirements would also allow physicians to apply for credentials at multiple hospitals at once, which leads into the next barrier to adoption.37
Licensure
Federal and state licensing laws have inhibited the adoption of telehealth since its inception. Policies vary across states, and these often require providers to obtain some form of licensure in each state that they wish to practice in. One of telehealth’s most impactful benefits is to connect patients and doctors at a distance. Licensure laws may limit the geographic footprints of physicians, while giving patients access only to doctors who have a current license in the state where they reside. Some states have tried to knock down the artificial barriers erected at the state boundary lines by joining the Interstate Medical Licensure Compact. In 2019, the Florida legislature passed a new law to authorize out-of-state health-care professionals to deliver telehealth services to local patients.38
Rural broadband gaps
Successful implementation of telehealth among rural communities requires the expansion of broadband internet access. Almost all forms of telehealth initiatives require an internet connection. While the lack of broadband access disproportionately affects rural areas, urban and suburban areas may also have subscribers who experience challenges getting online, like the cost of service. Without access to high-speed broadband networks, a large portion of rural populations will be challenged to partake in virtual medical care.
Existing health disparities
Along the same line, health disparities, especially among low-income populations and communities of color, may make it more difficult to access telehealth services. These phenomena often correlate with poverty, geographic isolation, and the likelihood of far less healthy alternatives for food and diet. Health disparities are also emboldened by disproportionate access to quality health-care facilities or the fragility of household economic resources, which deters vulnerable populations from seeking initial and follow-up care. Among medically marginalized communities, the hospital emergency room or urgent care centers tend to be the first options for treatment, resulting in exorbitant patient expenses which are reasons not to see a doctor in the future.
Removing barriers to telehealth adoption and use may be effective for members of vulnerable populations who also have exponential access to smartphones. Moreover, by waiving copayments for telehealth visits or implementing waivers to purchase the necessary prerequisites to support telehealth use (i.e., data plans, smartphones, or internet access), quality care would be available to an entire population who may have previously not considered telehealth as a viable platform to receive medical care.39 Enhancing consumer education of telehealth platforms among these groups also plays a role in reducing the distrust often associated with these modes of service.
“While health centers can motivate providers to adopt telehealth by providing financial incentives, organizational culture shifts are fundamental in embracing telehealth.”
Generally, states have attempted to provide relief to all or some of these barriers, but the efforts of their regulators alone are not enough to persuade providers and health systems to invest the time, energy, and money to offer telehealth services. Consequently, state or federal public policies must incentivize providers and health-care systems to be more favorable to telehealth adoption. For example, offering financial incentives for providers to adopt telehealth may increase usage—much like the recent waivers granted under COVID-19. While health centers can motivate providers to adopt telehealth by providing financial incentives, organizational culture shifts are fundamental in embracing telehealth.
Federal versus state execution of telehealth
The exertion of authority at the various levels of government can exacerbate some or all these barriers. While the federal and state governments have their hands in regulating the use of telehealth in some capacity, a lack of uniformity between these entities can create hesitation among patients, providers, or insurers to adopt telehealth. Moreover, within branches of government, the absence of consensus further stalls implementation.
Generally, federal laws have either been permissive or dismissive of telehealth provisions. Historically, the federal government has been involved in regulating telehealth initiatives within the Medicare program. But Medicare has been slow to change restrictive standards for the use of telemedicine. For example, following outdated standards created before the rise of telehealth, Medicare restricts reimbursement of this practice to those in rural areas and only to be performed at authorized “originating sites,” which excludes a patient’s home.40 More recent guidance from the federal government attempted to extend the use of telemedicine to more patients by expanding services that could be reimbursed within Medicare to include kidney care and acute stroke. Furthermore, accountable care organizations were provided with more flexibility to pay for telehealth services in additional locations such as one’s home. But overall, restrictions on what Medicare can pay for continues to hinder the usage telehealth practices.
Related Content
2020


Realizing the cost-savings and quality-of-care benefits from telehealth requires targeted policies at the appropriate levels of government. To this end, it is instructive to review the history of health-insurance markets to understand how their regulation and administration are divided between state and federal government. The federal government runs health-insurance programs for specific groups, including employees, veterans, and senior citizens, among others. Programs run exclusively by federal agencies include Tricare for military service members and their families, the Veterans Health Administration for veterans, and Medicare for senior citizens aged 65 and older, younger individuals with disabilities, and those with end-stage renal disease. These groups represent only 15% of the American population, and their health needs may not generalize to a broader population.41 Federal telehealth rules can also conflict with state-run programs, as in the case of Medicare limiting its use to rural areas while most state regulations contain no such geographic coverage limitations.42
In some cases, states share responsibility with the federal government for health-insurance programs, particularly those targeted to low-income households. States regulate private insurance markets besides mean-tested programs. The matter of state regulation of insurance was settled in 1945 by the McCarran-Ferguson Act, which effectively created 50 state markets for private health insurance after adoption by Congress. By then, the IRS had declared employee health-care benefits tax exempt, incentivizing the purchase of private insurance in statewide markets.43 The establishment of Medicaid in 1965 empowered states to extend health insurance to certain low-income groups, and the ACA expanded Medicaid eligibility to adults earning up to 138% of the poverty line. Between Medicaid and private insurance, over three-quarters of Americans purchase health insurance regulated at the state level.44 But these initial laws, in many respects, have led to the observed fragmentation in health-care regulation, which are points made in the next section.
Incongruencies in states’ telehealth administration
State telehealth laws frequently note that no two states have the same regulations when it comes to coverage and payment.45 States range from having no telehealth parity laws that specify which telehealth services are covered and their reimbursement rate, to having full coverage and payment parity for telehealth services. Such variables in state administration contribute to differences among telehealth laws across states. Further, state laws often do not place geographic restrictions on telehealth coverage.
“State telehealth laws frequently note that no two states have the same regulations when it comes to coverage and payment.”
Among health-care professionals, states also act as payers of insurance, both for their own employees and for the 21% of Americans who use Medicaid.46 In addition to insurance regulators that set rules for the private markets, state Medicaid agencies establish rules for how beneficiaries can use telehealth services. Most states have similar telehealth rules for Medicaid and private payers, but there are some exceptions. For instance, private insurance can generally reimburse for telehealth when the patient is at work or at home, while several Medicaid state guidelines specify that care must be delivered in a qualified health-care facility to be reimbursed.47
From a policy perspective, 50 state legislatures have more leeway to innovate in terms of the provision of health care than does Congress. States also hold the authority to regulate health insurers, and there are also fewer patients served in each state-run health-care program. Unfortunately, there are few transfers of learning across state governments—especially in the areas of successes and failures and the facilitation of policies across state borders.
Though this list is not exhaustive, many states use managed care organizations (MCO) to administer benefits for Medicaid recipients. The state normally pays MCOs on a fixed, per-member, per-month rate. This means that the MCO’s profit margin comes from administering successful care for the individuals enrolled in their plans below the total allotment that the MCO receives from the state. Incorporating cost-effective telemedicine visits is one-way that MCOs are attempting to lower costs, since there isn’t a need to be reimbursed separately for telemedicine when a patient’s care is paid for on a capitated monthly rate. Many of these MCOs also offer private insurance plans. While it’s beyond the scope of this paper, opportunities exist to explore MCOs’ use of telehealth and its effective incorporation into private plans and among all providers, regardless of who is paying for the service.
State benefits to patients, providers, and payers
The authors believe that state regulation of telehealth services can bring leverage to patients who prefer to see their local health-care providers remotely. Within state borders, telemedicine can expand the geographic area that a doctor and hospital can serve, and patients living in rural areas would not need to travel for routine consultations with primary-care physicians or specialists.
Telehealth services supplementing in-person care can provide more frequent access to care than either via telehealth or in-person visits. Providers also benefit from state-level regulation, since doctors primarily serve local patients, are reimbursed by state-licensed health insurers, and are licensed by state medical boards. Further, states define standards of care for its medical professionals. Doctors must navigate both their professional scope of practice as well as state insurance-reimbursement rules to offer telehealth services.
Finally, private health insurance is already sold and regulated at the state level, which substantiate its role at the epicenter of health policy. Payers can decide how telehealth can help them meet their coverage obligations under state regulations.48 In addition to working with in-network providers, some payers have contracted with third-party providers to provide telehealth services to their members.49
State roadblocks
However, telehealth implementation at the state level faces additional obstacles, despite their suitability for more customized services. Though 50 state governments can try many different approaches simultaneously, this can also delay the diffusion of telehealth services. Meeting requirements of 50 state health-insurance markets and medical boards delays the nationwide availability of new telehealth services. States also vary greatly in size and population. For example, a doctor offering a telehealth service in California or Texas can cover many more people over a larger area than a doctor in New Hampshire or Vermont. Incentives to adopt telehealth may be smaller in states with fewer patients to serve.
In a report on telemedicine adoption in North Carolina, Katherine Restrepo outlined several potential solutions to telehealth adoption across states.50 One is expanding the number of states that have signed the Interstate Medical Licensure Compact, which streamlines the process for physicians applying for licensure in other member states. However, this still limits telehealth practice based on state licensure. Another solution would be a federal law that designates the provider’s location as the location in which care takes place for the purposes of licensure and payment. This would preserve the authority of state medical boards to grant licenses, while allowing physicians to treat patients remotely in other states.
Though states regulate private insurance markets, the Employee Retirement Income Security Act (ERISA), passed by Congress in 1974, exempts employer-funded health-care plans from state insurance regulations. Rather than buy employee health insurance from a third-party vendor, it can be cost effective for larger firms to spread out medical expenses over their many employees. In 2019, 61% of covered workers had an insurance plan that was wholly or partially funded by their employer, and this figure rises to 86% for firms with more than 1,000 workers.51 Telehealth services for these covered employees must comply with ERISA, either through their health plans or in separate filings for standalone benefits.52 This high percentage of workers with plans that are exempt from state regulations complicate efforts to promote telehealth adoption through state law.
Connecting patients and providers
Pursuing telehealth policy changes at the state level appears to reach the greatest number of people because much of the power to regulate health-care insurance has been delegated to states. While the federal government can promote telehealth coverage in the population it serves by changing reimbursement rules for Medicare and by setting minimum coverage standards for Medicaid, state insurance regulators, Medicaid agencies, and medical boards can all change rules for practice, coverage, and reimbursement to promote greater use of telehealth services for those not insured through federal programs.
“Not only is the federal government often paralyzed by partisanship, it has far less autonomy over the state insurance markets that will regulate the use of telemedicine.”
Not only is the federal government often paralyzed by partisanship, it has far less autonomy over the state insurance markets that will regulate the use of telemedicine. Moreover, policy is most effective when it is administered as close as possible to the people that are affected by it. Therefore, states, in close conjunction with their local providers, insurers, and patients should lead in reforming telehealth regulations.
The reform is also needed for two reasons: first, because of how inconsistent regulations are among the states and between state governments and the federal government; and second, because some of the regulations currently in place may inhibit more widespread telehealth adoption.
The impact of state parity laws
A case in point is related to the adoption and administration of state parity laws, which can affect both coverage and costs. As part of the research, we conducted a 50-state analysis to show the full spectrum of how widely states vary in their telemedicine regulations, from private-payer parity laws to those that are more robust. What we found is that 13 states have no private payer telemedicine parity laws. Of the states that do mandate some form of parity, seven states mandate partial coverage of telemedicine, specifying which services must be covered; 19 states mandate full coverage parity, where coverage is the same for services delivered via telemedicine and in-person; and 11 states mandate full coverage and payment parity, where covered services must be reimbursed at the same rate as an in-person visit. (See Figure 1 below.) Table 1 offers the information in text form and provides more clarification to Figure 1’s illustration of national parity laws.
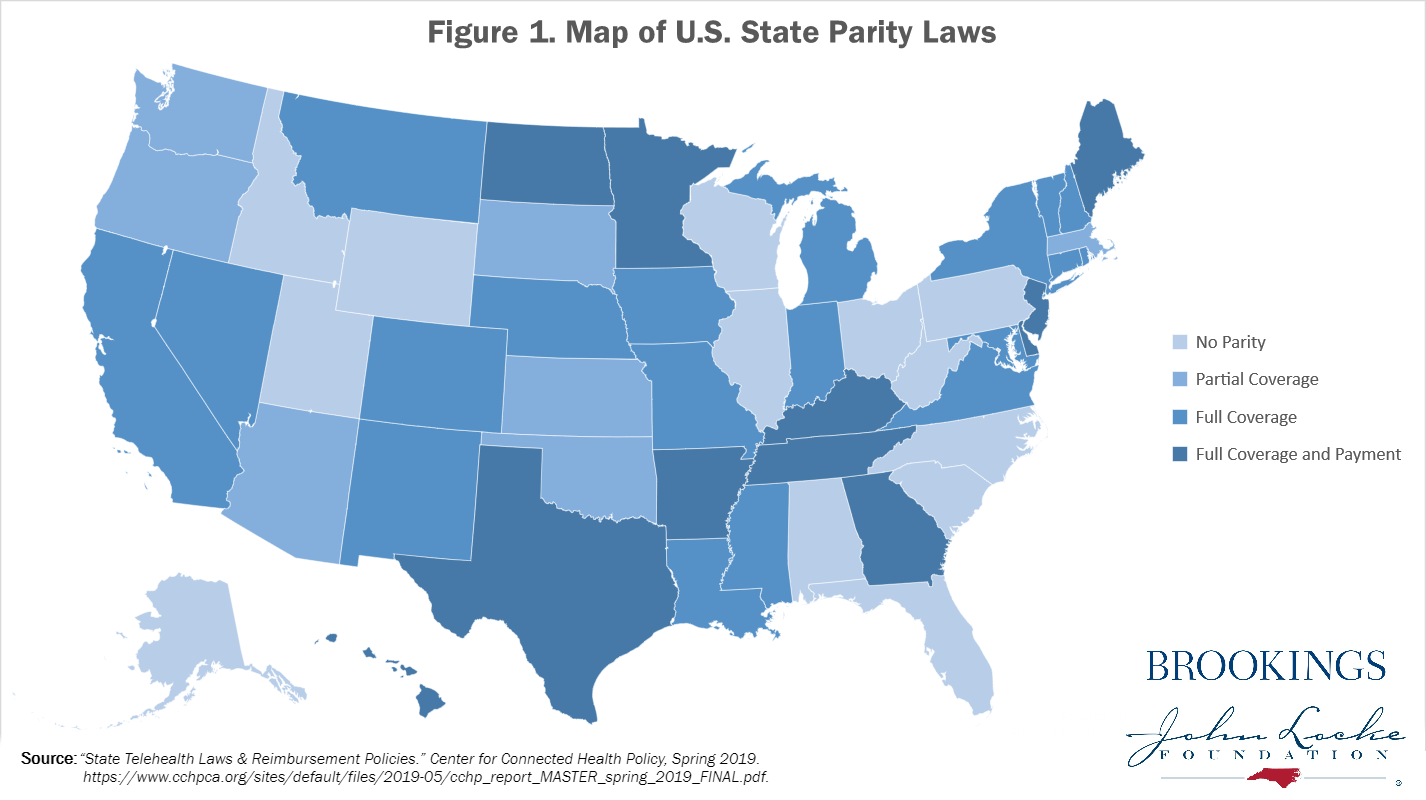
Table 1: Parity Law Status by State
| State Name | No Parity | Partial Coverage | Full Coverage | Coverage & Payment |
| Alabama | X | |||
| Alaska | X | |||
| Arizona | X | |||
| Arkansas | X | |||
| California | X* | |||
| Colorado | X** | |||
| Connecticut | X* | |||
| Delaware | X | |||
| Florida | X | |||
| Georgia | X* | |||
| Hawaii | X* | |||
| Idaho | X | |||
| Illinois | X | |||
| Indiana | X | |||
| Iowa | X | |||
| Kansas | X* | |||
| Kentucky | X** | |||
| Louisiana | X† | |||
| Maine | X | |||
| Maryland | X | |||
| Massachusetts | X | |||
| Michigan | X | |||
| Minnesota | X | |||
| Mississippi | X | |||
| Missouri | X** | |||
| Montana | X | |||
| Nebraska | X** | |||
| Nevada | X | |||
| New Hampshire | X** | |||
| New Jersey | * | X* | ||
| New Mexico | X | |||
| New York | X | |||
| North Carolina | X | |||
| North Dakota | X | |||
| Ohio | X | |||
| Oklahoma | X | |||
| Oregon | X* | |||
| Pennsylvania | X | |||
| Rhode Island | X*,** | |||
| South Carolina | X | |||
| South Dakota | X | |||
| Tennessee | X | |||
| Texas | X** | |||
| Utah | X | |||
| Vermont | X | |||
| Virginia | X | |||
| Washington | X*** | |||
| West Virginia | X | |||
| Wisconsin | X | |||
| Wyoming | X | |||
| Table key | ||||
| Symbol | Note | |||
| * | Coverage parity subject to terms and conditions of the contract. | |||
| ** | Coverage parity language states “insurers payers cannot deny exclude coverage solely because the service is provided through telemedicine.” | |||
| *** | “Services must be considered an essential health benefit under the ACA…” | |||
| † | Payment must be at least 75% as it would be for in-person service. | |||
| Source: “State Telehealth Laws & Reimbursement Policies.” Center for Connected Health Policy, Spring 2019. https://www.cchpca.org/sites/default/files/2019-05/cchp_report_MASTER_spring_2019_FINAL.pdf. | ||||
While state parity laws have been implemented with good intention to attempt a more uniform use and regulation of telehealth reimbursement, payment parity laws in practice may not produce the intended effects. The main problem with payment parity laws is that they are contradictory to telehealth’s cost-effectiveness. If telehealth can help reduce costs of using the health-care system and reduce doctor visits, it is contradictory to mandate that a service provided through telehealth be paid for at the same rate as if it were provided in a doctor’s office.
“The main problem with payment parity laws is that they are contradictory to telehealth’s cost-effectiveness.”
Similarly, coverage parity laws may also have unintended consequences for telemedicine adoption. Effective telehealth initiatives will have support from the provider, insurer, and patient. By mandating the coverage of telemedicine into health plans, private insurers now face additional regulations that they must factor into their benefit-plan designs. Furthermore, providers may favor slower adoption or trials to test out telehealth initiatives. As described throughout the paper, the practice of telehealth is consumer-driven by nature. Mandating parity requirements reduces the freedom that insurers and providers have to determine the proper role and payment of telehealth practices.
In the case of state parity laws, for example, a substantial amount of variability exists among the regulations that govern this practice. Often, the laws may not include all the possible modalities by which one could use telehealth technology, which limits what can be considered applicable to telemedicine laws and lead to the exclusion of some useful new telehealth practices. Further, health-care laws are not written in such a way to account for future use of undiscovered telehealth practices. Thus, it may be the case that a parity law is written to only include the current forms of the technology. Again, these laws, which are intended to encourage the use of telemedicine, may hinder the uptake because the regulations won’t be able to keep up with the technology.
Under the mitigation plan of COVID-19, many states are relying upon existing state parity laws to recoup reimbursement for eligible expenses, especially considering the Medicare waivers. Herein, the legislation makes it possible for payers to reimburse providers at parity for visits conducted via telehealth during the coronavirus outbreak. However, will this be the case when the crisis mode of the pandemic subsides?
Going into the next phase of mitigation, telehealth services should be maintained, but without state payment-parity laws. Under normal circumstance, these laws are contrary to telehealth’s cost-effective nature because health-care providers would operate based on their average patient volume. Given the lack of feasibility to see a doctor in person due to imposed stay-at-home orders, public-health officials have recommended postponing any procedures or doctor visits that can wait. Under typical patient volumes, providers would have a steady flow of in-person visits to combine with telehealth visits. But under reduced patient volumes mandated by the government, paying these providers at parity makes sense to help keep them afloat since typical patient volumes are artificially suppressed. But again, when these patient volumes aren’t artificially suppressed, will the innovation be stifled largely due to the lack of demand? This question is of highest importance if the continuity of telehealth services will be maintained.
Telehealth and COVID-19
Clearly, the world’s experience with the recent COVID-19 pandemic has shown the value of telemedicine in limiting the spread of disease while ensuring access to medical expertise. For patients who present symptoms of a possible infection, telehealth will not replace virus testing to determine the presence of coronavirus. However, screening questions and remote consultation with a physician can ascertain a patient’s need for additional treatment without compromising others in near proximity. Avoiding contact is critical for halting the spread of disease, so diverting non-urgent cases from hospitals essentially frees up resources for patients with the most critical need. Telehealth can also be useful in protecting elderly patients and medically vulnerable populations by facilitating interactions between providers and patients in safer environments.
“[T]he world’s experience with the recent COVID-19 pandemic has shown the value of telemedicine in limiting the spread of disease while ensuring access to medical expertise.”
The novel coronavirus was an unlikely accelerant for telehealth use in the U.S. The mandatory appeals for social distancing—maintaining six feet between individuals in public places—made technology a useful tool for adherence to these principles. However, governing bodies at the federal and state levels relaxed many of the regulations to fully unleash telehealth during the outbreak—some of which may be returned after this public-health crisis. As mentioned, the federal government and some states expanded the definitions that govern the use of telehealth, including the types of providers who could bill the government for telehealth services, and increased the devices and locations for which a patient could use telemedicine. The federal government and some states recognized out-of-state licenses for the purposes of telehealth. This means that a licensed provider in Virginia would not have to get a separate North Carolina license just to see a patient remotely.
In addition to relaxing regulations, the federal government increased funding for new telehealth initiatives. The $2 trillion Coronavirus Aid, Relief, and Economic Security (CARES) Act passed by Congress included $200 million for the Federal Communications Commission to expand telehealth services across the country. More specifically, health-care providers will be able to apply these funds toward medical devices and telecommunications equipment that enable remote care as part of the COVID-19 Telehealth Program.53 A further $100 million from the Universal Service Fund administered by the FCC will finance a three-year Connected Care Pilot program to subsidize internet connectivity for health-care providers. The additional federal funding recognizes that telehealth can play a role in the short-term pandemic response as well as long-term provision of health care in the U.S.
Thus, the coronavirus outbreak not only increased the awareness of this technology, but also provided doctors and patients with easier access to use it both physically and financially. Both impacts should bode well for telehealth’s use in the future. But readers should understand that because of the political nature of health care in the U.S., the benefits could be easily wiped away.
Even in the absence of the coronavirus, telehealth should evolve as a common practice in medicine. While the coronavirus bolstered its critical use, it was more deregulation that made it readily available to providers and patients across state lines, many of which were barriers identified earlier in the paper. Going forward, the real work begins now as COVID-19 has revealed its adoption and use, suggesting that a reversal of certain restrictions and an examination of state parity laws should happen.
The recommendations in the final part of this paper attempt to harmonize what should begin to be the norm around the use of technology in health care. More specifically, when the nation returns to some level of normalcy, how will a health-care environment driven by digitized health services be supported and maintained, especially if there is a shift in presidential leadership? The proposed recommendations offer some framing for the delivery of such services and the role of states—which have been the primary mitigators of local health options in ensuring telehealth’s continuity after the pandemic.
Policy recommendations
The U.S. health-care system has only begun to scratch the surface regarding the integration of telehealth practices into the traditional delivery of health care. This final section offers a list of policy priorities that would create a more uniform and functional regulatory environment for patients, providers, and insurers around telehealth in the future.
- Data on COVID-19 telehealth administration and programs must be collected and analyzed.
Journalists and researchers have begun to explore the increased value of telehealth after COVID-19, suggesting that Congress may look to more utilization versus reimbursement models in making the services more widely available.54 In fact, some have suggested that continued adoption and use of telehealth could help hospitals buffer the losses due to the coronavirus, due in part to the waivers that the federal government has instituted.55 But moving forward, it will be incumbent upon the federal government, associations representing the health-care industry, and the private companies that comprise the health-care sector to amass data on how telehealth was used during the pandemic, identifying the opportunities and blind spots in its use. On the latter point, many doctors were already providing “remote” services via telephone. Going toward some level of permanency, would this constitute an eligible service for people who may not have access to an internet-enabled device or digital health application or tool?
As telehealth was operationalized from a “boots on the ground” model during COVID-19, a term familiar among the medical community in times of crises, state and federal legislators should be able to showcase the outcomes to patients, hospitals, and insurance companies as it evolves from “national pilot” to one that is fully utilized by the medical community. Some analysts have called for more methodical and uniform data collection among providers, which may or may not have occurred during an immediate response to the coronavirus. But if the technology is going to be effectively deployed, or if changes are going to be made around its use, it is imperative that a sufficient system for data capture happen now and extend some time after the peak periods of mitigation to determine its effectiveness and potentially make claims to its efficacy going forward.
- Regulatory flexibility should be built into telehealth to accommodate the range of use cases.
In addition to collecting data on telehealth’s use, the current regulations (particularly those that were waived) and the guidance going into COVID-19 will need to be assessed by Congress—before any changes or a return to legacy regulations are made. As has been documented, large gaps in the consistency among the states was present before the outbreak and will still be there absent of legislative fixes at both the state and federal levels. For example, something as basic as defining a telehealth “visit” can differ between states based on geographic and site restrictions. If the U.S. reverts to its long-term memory over the statutes that were in place, the country will likely negate the lessons learned under a deregulatory, streamlined framework over the last few months. Moving forward, more flexibility in telehealth delivery (e.g., the devices used, the methods, etc.) may drive better consistency in the administration of services and support the next wave of innovation in the health-care field.
“[T]elehealth regulations—especially those at the state-level—must be drafted with a broad eye toward the future, being as flexible as possible to incorporate existing and emerging modalities of the future.”
That is, telehealth regulations—especially those at the state-level—must be drafted with a broad eye toward the future, being as flexible as possible to incorporate existing and emerging modalities of the future. As states codify specific types of telehealth practices that can be used and reimbursed in medical practices, such a limited scope may hinder the evolution of technology into health care because innovation will move faster than the laws can be updated. In fact, regulation should more so be looking at patient guardrails, including privacy and data security, something that will become more critical with increased data flows between doctors and patients.
- Telehealth services should be utilized for primary care to reduce service redundancies.
The importance of one’s access to primary care is hard to overstate. For many patients, their primary-care doctor will be the health professional that they see the most. If questions around utilization emerge around telehealth, primary care should be flagged as a priority application. First, patients may be the most comfortable with and trustworthy of their primary-care provider, making the introduction of video conferencing or remote monitoring easier for the doctor. Second, due to the lack of primary-care support for the medically underserved in rural communities and among people of color, telehealth can be extremely beneficial—even for older Americans. Telehealth visits and other telehealth modalities, such as remote patient monitoring, can bring health care into the homes of patients who often face additional barriers to having more than enough (or any) insurance and health access.
Further, adding telehealth options into a medical practice can expand the number of new patients for a provider. If patient and claims volume increase, the physician would have greater flexibility to interact with patients. Providers will also be able to manage patient visits and office resources more efficiently by coordinating visits through telehealth, contributing to reduced wait times and fewer cancellations for in-person visits.
- States should be empowered to move away from parity models to reduce the cost of telehealth services.
To increase the use of telehealth among providers and raise the value for patients, states should not sign on to parity models for reimbursement, which can stagnant their abilities to embrace a wide range of technologies and modalities as eligible services. Many of the existing state parity laws are implemented with good intentions, but lack of enforcement. Parity laws also mandate the same reimbursement of a “visit” that happens via telemedicine to that of one made in-person with a medical professional. Because the delivery costs are lower, telehealth services should be treated as such, and potentially coordinated between states to ensure their wide acceptance. As telehealth was subjected to parity during the coronavirus outbreak, the times dictated such an intervention, especially in the absence of a reasonable model for reimbursement. But people are already paying too much in health-care expenses with many people going without any type of coverage. Telehealth has direct and indirect benefits to both providers and the institutions in which they work. As a cost saver, the services should be treated as such and not encumbered by uneasy expenses that deter patients from their use, especially if they are subjected to the same cost structure as coming into a facility.
- Telehealth services should be available to the medically underserved.
What the handling of the medical stresses induced by the coronavirus have revealed is that health disparities disproportionately impact people of color, who are more likely to have chronic pre-existing conditions like diabetes and heart disease. Older patients are similarly vulnerable and may not have the resources or ability to travel to their doctors. For rural Americans, quality of life may be dictated largely by their access to services, which in some cases may be miles and hours away. These populations and others, including people with disabilities, suggest that telehealth services should be expanded to target these underserved groups, where the fragmentation of services, cost, and geography can equate to well-being.
Unfortunately, many of these populations reside in locations or are individually subjected to the challenges of not having broadband access due to the cost or availability. In this case, it is important for federal and state governments to promote universal access to high-speed broadband through expanded infrastructure or through the federal Lifeline program, which provides individuals with discounted mobile or broadband service. The FCC’s Connected Care Pilot program can also help, depending on how fast $100 million dollars of funding over three years will connect low-income Americans and veterans to broadband for the purpose of telehealth. Another potential option for expanding broadband access involves creating a new broadband triple-play ecosystem, aligning hospitals, schools, and libraries into a telehealth-care hub.56 Libraries often have the fastest broadband connections in the community, and they could be a key planning source and funding partner in the expansion of broadband services for telehealth use.57
These types of programs should not be introduced and adopted at times of pandemics. Rather, the U.S. needs to work toward closing the digital divide so that all Americans can connect to a medical provider to address new and chronic conditions in a more methodical way.
- Innovation, privacy, and data security in telehealth services should be the norm.
Emerging technologies like AI and digital health devices have the potential to expand access to health care without negatively impacting patient privacy. Going forward, it is important to tether the conversations around the need for U.S. federal privacy legislation with telehealth services. Debates around the importance of encryption are equally important, especially as more individuals engage in personal conversations with doctors over their internet-enabled devices. Seemingly, telehealth services will generate large quantities of data that must be protected when moving between patient and provider. HIPAA privacy protections should still apply to these interactions, and the technical cadence that encourages privacy-by-design should be encouraged by private sector device and apps makers.
“Going forward, it is important to tether the conversations around the need for U.S. federal privacy legislation with telehealth services.”
Data security is also of high priority in securing sensitive, personal health data. Why encryption, without potential back doors for invasive surveillance, matters is because it secures health data on a variety of applications and devices, which will be important in the forthcoming conversations on digital health. In the end, when the U.S. emerges from the mitigation of COVID-19, these questions and issues must be raised to ensure that both patients and providers face minimal risk in the use of these tools.
Conclusion
Telehealth regulations have been debated over decades, starting with the technology’s early applications when it was restricted to an SMS text or phone call. Today, telehealth has proven itself a viable supplement to an already strained health-care system, where both medical providers and patients are seeking timely, effective, and robust tools for early detection, primary care, and long-term evaluation. While progress was being made before the coronavirus outbreak to adopt telehealth in states, the pandemic not only demonstrated its worth but also proved it necessary to avert larger meltdowns in hospital systems and among medical professionals—even those whose work was stopped due to social distancing.
The world will probably not return to the normalcy it once experienced before COVID-19—and neither should health care. As Congress is charged with re-evaluating the leniencies permitted to health-care providers during this crisis, federal lawmakers should also see the benefits. The same holds true for states that will need to reconsider lifting boundaries on telehealth services to accelerate its transformational capabilities for patients and doctors.
Acknowlegements
The authors would like to thank Shezaz Hannan, Bhaargavi Ashok, and Lia Newman for their research support.
The Brookings Institution is a nonprofit organization devoted to independent research and policy solutions. Its mission is to conduct high-quality, independent research and, based on that research, to provide innovative, practical recommendations for policymakers and the public. The conclusions and recommendations of any Brookings publication are solely those of its author(s), and do not reflect the views of the Institution, its management, or its other scholars.
The John Locke Foundation employs research, journalism, and outreach programs to transform government through competition, innovation, personal freedom, and personal responsibility. The Foundation seeks a better balance between the public sector and private institutions of family, faith, community, and enterprise.
Authors



-
Footnotes
- Kaiser Permanente. “Why Telehealth – Benefits & Barriers to Adoption.” Accessed April 27, 2020. https://business.kaiserpermanente.org/insights/telehealth/why-benefits-barriers.
- Health Affairs. “National Health Care Spending In 2018: Growth Driven By Accelerations In Medicare And Private Insurance Spending.” Accessed April 8, 2020. https://www.healthaffairs.org/doi/abs/10.1377/hlthaff.2019.01451?journalCode=hlthaff.
- Andrea M. Sisko et al., “National Health Expenditure Projections, 2018–27: Economic And Demographic Trends Drive Spending And Enrollment Growth,” Health Affairs 38, no. 3 (March 2019): 491–501, https://doi.org/10.1377/hlthaff.2018.05499.
- Kaiser Permanente. “Why Telehealth – Benefits & Barriers to Adoption.” Accessed April 27, 2020. https://business.kaiserpermanente.org/insights/telehealth/why-benefits-barriers.
- Thorpe, Kenneth E., Kathy Ko Chin, Yanira Cruz, Marjorie A. Innocent, and Lillian Singh. “The United States Can Reduce Socioeconomic Disparities By Focusing On Chronic Diseases.” Health Affairs. Accessed April 16, 2020. https://www.healthaffairs.org/do/10.1377/hblog20170817.061561/full/.
- Sukel, Kayt. “Dealing with the Shortage of Rural Physicians.” Medical Economics, August 29, 2019. https://www.medicaleconomics.com/news/dealing-shortage-rural-physicians.
- Landi, Heather. “Trump administration opens up access to telehealth services during coronavirus outbreak.” Fierce Healthcare, March 17, 2020, https://www.fiercehealthcare.com/payer/trump-administration-opens-up-access-to-telehealth-services-during-coronavirus-outbreak
- Enlund, Sydne. “Increasing Access to Health Care Through Telehealth.” Accessed October 3, 2019. http://www.ncsl.org/research/health/increasing-access-to-health-care-through-telehealth.aspx.
- Kuziemsky, Craig, Anthony J. Maeder, Oommen John, Shashi B. Gogia, Arindam Basu, Sushil Meher, and Marcia Ito. “Role of Artificial Intelligence within the Telehealth Domain.” Yearbook of Medical Informatics 28, no. 1 (August 2019): 35–40. https://doi.org/10.1055/s-0039-1677897.
- OECD Data. “Health Spending.” Accessed April 8, 2020. https://data.oecd.org/healthres/health-spending.htm.
- Inserro, Allison. “Healthcare Spending Driven by Price, Not Utilization: JAMA Study.” AJMC, March 14, 2018. https://www.ajmc.com/newsroom/healthcare-spending-driven-by-price-not-utilization-ijamai-study-.
- O’Neill, Daniel P., and David Scheinker. “Wasted Health Spending: Who’s Picking Up The Tab?” Health Affairs, May 31, 2018. https://www.healthaffairs.org/do/10.1377/hblog20180530.245587/full/.
- OECD.Stat. “Health Status.” Accessed April 8, 2020. https://stats.oecd.org/Index.aspx?DataSetCode=HEALTH_STAT.
- HealthCare.gov. “Affordable Care Act (ACA) – HealthCare.Gov Glossary.” Accessed April 8, 2020. https://www.healthcare.gov/glossary/affordable-care-act/.
- Tolbert, Jennifer, Kendal Orgera, Natalie Singer, Anthony Damico. Published: Dec 13, and 2019. “Key Facts about the Uninsured Population.” The Henry J. Kaiser Family Foundation (blog), December 13, 2019. https://www.kff.org/uninsured/issue-brief/key-facts-about-the-uninsured-population/.
- Berchick, Edward R, Emily Hood, and Jessica C Barnett. “Health Insurance Coverage in the United States: 2017.” U.S. Department of Commerce, September 2018, 44.
- The Henry J. Kaiser Family Foundation. “Health Insurance Coverage of the Total Population,” December 4, 2019. https://www.kff.org/other/state-indicator/total-population/.
- “U.S. Senate: U.S. Senate Roll Call Votes 111th Congress – 1st Session,” Accessed September 6, 2019, https://www.senate.gov/legislative/LIS/roll_call_lists/roll_call_vote_cfm.cfm?congress=111&session=1&vote=00395.
- Redhead, C. Stephen, and Janet Kinzer. “Legislative Actions in the 112th, 113th, and 114th Congresses to Repeal, Defund, or Delay the Affordable Care Act.” Congressional Research Service, February 7, 2017, 26.
- Levinson, Daniel R. “HealthCare.Gov: CMS Management of the Federal Marketplace” Office of the Inspector General, U.S. Department of Health and Human Services, February 2016. https://oig.hhs.gov/oei/reports/oei-06-14-00350.pdf.
- Wicklund, Eric. “Hospital’s Telehealth Program Reduces ER Visits, Treatment Costs.” mHealthIntelligence, January 25, 2019, https://mhealthintelligence.com/news/hospitals-telehealth-program-reduces-er-visits-treatment-costs.
- Ibid.
- Cheney, Christopher. “Cost Savings for Telemedicine Estimated at $19 to $120 per Patient Visit.” Health Leaders, May 7, 2019. https://www.healthleadersmedia.com/welcome-ad?toURL=/clinical-care/cost-savings-telemedicine-estimated-19-120-patient-visit.
- Wicklund, Eric. “Telehealth Targets a Niche in Mental Health Care for Urban Youths.” mHealthIntelligence, January 3, 2018. https://mhealthintelligence.com/news/telehealth-targets-a-niche-in-mental-health-care-for-urban-youths.
- Restrepo, Katherine. “The Case Against Telemedicine Parity Laws.” John Locke Foundation, January 15, 2018. https://www.johnlocke.org/research/telemedicine/.
- (pg. 9) World Health Organization, ed. Telemedicine: Opportunities and Developments in Member States. Global Observatory for EHealth Series 2. Geneva, Switzerland: World Health Organization, 2010.
- Ibid.
- “About Telemedicine – ATA Main.” Accessed April 8, 2020. http://legacy.americantelemed.org/about/about-telemedicine.
- HealthIT.gov. “What Is Telehealth? How Is Telehealth Different from Telemedicine?” Accessed April 8, 2020. https://www.healthit.gov/faq/what-telehealth-how-telehealth-different-telemedicine.
- NEJM Catalyst. “What Is Telehealth?,” February 1, 2018. https://catalyst.nejm.org/doi/full/10.1056/CAT.18.0268.
- U.S. Food and Drug Administration. “Digital Health.” FDA, March 26, 2020. https://www.fda.gov/medical-devices/digital-health.
- American Medical Association. “Digital Health Implementation Playbook.” 2019. https://www.ama-assn.org/system/files/2020-04/ama-telehealth-implementation-playbook.pdf
- Lin, Ching-Ching Claire, Anne Dievler, Carolyn Robbins, Alek Sripipatana, Matt Quinn, and Suma Nair. “Telehealth In Health Centers: Key Adoption Factors, Barriers, And Opportunities.” Health Affairs (Project Hope) 37, no. 12 (2018): 1967–74. https://doi.org/10.1377/hlthaff.2018.05125.
- “Telehealth Policy Barriers 2019,” Center for Connected Health Policy, accessed October 3, 2019, https://www.cchpca.org/sites/default/files/2019-02/TELEHEALTH%20POLICY%20BARRIERS%202019%20FINAL.pdf.
- Restrepo, Katherine. “The Case Against Telemedicine Parity Laws.” John Locke Foundation: Raleigh, NC, January 15, 2018. https://www.johnlocke.org/research/telemedicine/.
- Ibid.
- eVisit. “Barriers to Telemedicine and Telehealth Adoption.” Accessed April 27, 2020. https://evisit.com/resources/barriers-to-telemedicine-and-how-to-solve-them/
- Scott, Jeff. “The Reality of Florida’s New Telehealth Law.” FL Medical, n.d., 5.
- Park, Jeongyoung, Clese Erikson, Xinxin Han, and Preeti Iyer. “Are State Telehealth Policies Associated With The Use Of Telehealth Services Among Underserved Populations?” Health Affairs 37, no. 12 (December 1, 2018): 2060–68. https://doi.org/10.1377/hlthaff.2018.05101.
- Wynne, Billy, and Josh LaRosa. “A Tell-All on Telehealth: Where Is Congress Heading Next?” Commonwealth Fund, May 16, 2019. https://doi.org/10.26099/rcdd-my07.
- Berchick, Edward R, Emily Hood, and Jessica C Barnett. “Health Insurance Coverage in the United States: 2017.” U.S. Department of Commerce, September 2018, 44.
- “Telehealth Private Payer Laws: Impact and Issues.” Center for Connected Health Policy, August 2017. https://www.milbank.org/wp-content/uploads/2017/08/MMF-Telehealth-Report-FINAL.pdf.
- Carroll, Aaron E. “The Real Reason the U.S. Has Employer-Sponsored Health Insurance.” The New York Times, September 5, 2017. https://www.nytimes.com/2017/09/05/upshot/the-real-reason-the-us-has-employer-sponsored-health-insurance.html.
- The Henry J. Kaiser Family Foundation. “Health Insurance Coverage of the Total Population,” December 4, 2019. https://www.kff.org/other/state-indicator/total-population/.
- “State Telehealth Laws & Reimbursement Policies.” Center for Connected Health Policy, Spring 2019. https://www.cchpca.org/sites/default/files/2019-05/cchp_report_MASTER_spring_2019_FINAL.pdf.
- The Henry J. Kaiser Family Foundation. “Health Insurance Coverage of the Total Population,” December 4, 2019. https://www.kff.org/other/state-indicator/total-population/.
- “Telehealth Private Payer Laws: Impact and Issues” Center for Connected Health Policy, August 2017. https://www.milbank.org/wp-content/uploads/2017/08/MMF-Telehealth-Report-FINAL.pdf.
- Ahn, Sandy, Sabrina Corlette, and Kevin Lucia. “Can Telemedicine Help Address Concerns with Network Adequacy? Opportunities and Challenges in Six States.” Urban Institute: Washington, DC, April 2016. https://www.urban.org/sites/default/files/publication/79551/2000736-Can-Telemedicine-Help-Address-Concerns-with-Network-Adequacy-Opportunities-and-Challenges-in-Six-States.pdf.
- “Telehealth Private Payer Laws: Impact and Issues.” Center for Connected Health Policy, August 2017. https://www.milbank.org/wp-content/uploads/2017/08/MMF-Telehealth-Report-FINAL.pdf
- Restrepo, Katherine. “The Case Against Telemedicine Parity Laws” John Locke Foundation: Raleigh, NC, January 15, 2018. https://www.johnlocke.org/research/telemedicine/.
- “2019 Employer Health Benefits Survey – Section 10: Plan Funding,” September 25, 2019. https://www.kff.org/report-section/ehbs-2019-section-10-plan-funding/.
- Waltman, Jessica. “Telemedicine Benefits Are Trending, But They Bring Compliance Considerations,” July 13, 2018. https://ktbenefits.com/2018/07/telemedicine-benefits-are-trending-but-they-bring-compliance-considerations/.
- Federal Communications Commission. “COVID-19 Telehealth Program,” April 8, 2020. https://www.fcc.gov/covid-19-telehealth-program.
- Lagasse, Jeff. “COVID-19 may permanently alter the telehealth landscape, from reimbursement to utilization.” Healthcare Finance, April 21, 2020. https://www.healthcarefinancenews.com/node/140009
- Ibid.
- Settles, Craig. “Health Care Hubs: The Future Of Telemedicine and Broadband.” Broadband Communities, February 2018. http://www.bbcmag.com/broadband-applications/health-care-hubs-the-future-of-telemedicine-and-broadband.
- Settles, Craig. “Libraries: Broadband Leaders of the 21st Century,” March 2016, 47.
The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).


