Domestic violence is sometimes called an “invisible epidemic.” Worldwide, 27% of all women experience physical or sexual intimate partner violence over their lifetimes. In the United States the figure may be as high as 41%. And even those statistics are surely underestimates—perhaps substantially so—given how dramatically underreported domestic violence is around the world.
With a problem so pervasive and damaging, we need to do everything we can to aid domestic violence survivors, and our new research shows that we are missing key opportunities.
Using new data from a large urban trauma center in Chicago, we document substantial under-reporting of domestic violence at the time of receiving medical care. Our analysis suggests that many women who receive treatment for their injuries in the emergency room (ER) do not disclose domestic violence victimization to medical personnel but do report to law enforcement within several days. This points to a missed opportunity to offer services and protection to domestic violence survivors earlier and in a more appropriate setting.
Using big data to identify domestic violence under-reporting
To understand domestic violence underreporting, our University of Chicago research team partnered with several city agencies in Chicago. We merged medical record data from emergency room visits to the University of Chicago Medical Center from 2008 through 2018 with information on crime victimization from the Chicago Police Department. The main analysis sample consists of both female and male patients, although below we also report results separately by gender. The matching was carried out in the most secure possible computing environment that meets the strictest patient confidentiality standards laid out by the Health Insurance Portability and Accountability Act of 1996. Only a subset of the research team had access to the data with identifying information, and only for purposes of matching the two datasets. Once the datasets were merged together, information that could be used to identify individuals was removed from the data used for the analysis. The rest of the research team only had access to this fully anonymous version of the dataset.
We focus this analysis on adult ER patients who had an X-ray. The data reveals a crucial point of failure in the city’s efforts to support survivors of domestic violence: 60 out of every 10,000 adults receiving an X-ray go on to report a domestic violence victimization to local law enforcement authorities within a few days of the ER visit. But only 5.5 out of 10,000 disclosed domestic violence to medical professionals in the ER (as measured by having an indication of domestic violence in the ER’s medical records).1 Figure 1 shows this disparity.
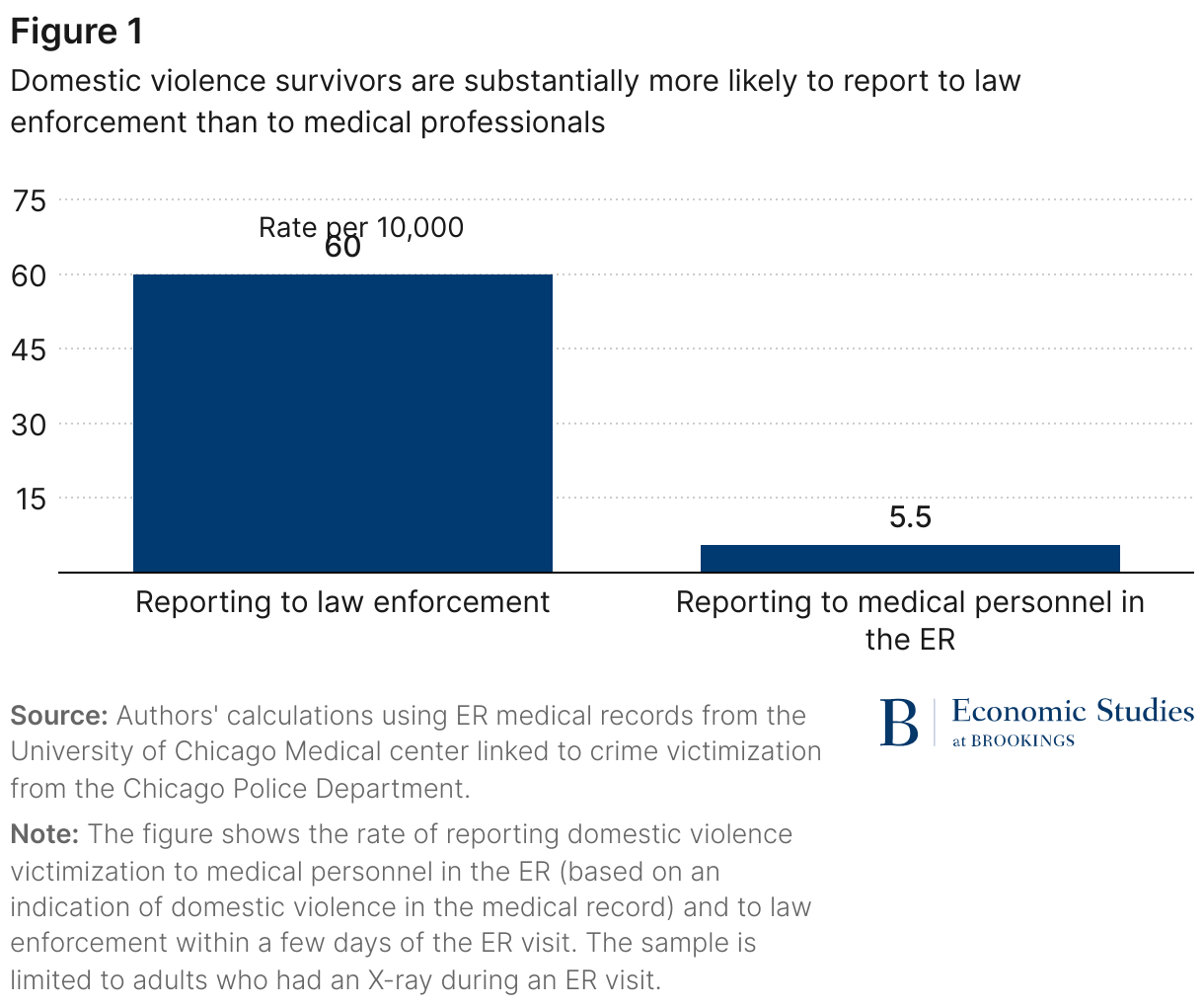
The results shown in Figure 1 are based on data for both female and male patients; the pattern is similar if we focus on female patients separately. The motivation to look separately by gender comes partly from gender differences in population prevalence rates and partly from differences in the nature of domestic violence-related injuries that women and men experience and the likelihood that such injuries require medical care. The rate of reporting domestic violence to law enforcement following an ER visit that involved an X-ray is higher for female patients than in the pooled sample (74 versus 60 per 10,000), as is the share that involve reporting domestic violence to medical staff (8 versus 5.5 per 10,000). Overall, the ratio of female patients that report to police versus medical staff is not that different from what we see for all patients pooled together (9 versus 12).
Missed opportunities
One implication of these findings is that many survivors are reporting to agencies—law enforcement—that are not well-equipped to handle complex medical and social needs of domestic violence survivors. Meanwhile, in most cases, institutions that might be better equipped to do this work—such as medical providers and their social service agency partners—do not know about these opportunities to help. Further, while the rate of reporting to law enforcement is higher than to medical professionals in the ER, almost half of survivors of domestic violence do not report the abuse to law enforcement either. That means the vast majority of domestic violence survivors are unknown to the social service agencies who might help.
Could medical providers be doing more to effectively identify people who have experienced domestic violence during visits to the ER? We find evidence that injuries in domestic violence cases are different from the average ER visit. Domestic violence-related visits are more likely, for example, to involve X-rays of certain body parts—such as elbows, forearms, hands, wrists, head, and neck—and are more likely to have the chief complaint for the visit recorded as “NA.”
Next steps to better connect domestic violence survivors to services
More research is needed to use the type of data we analyze here to see if there are identifiable patterns in medical records that indicate domestic violence involvement. Service providers, advocates, and other experts in the domestic violence field could then use that information to improve systems that connect survivors to supportive, protective services. Patients whose case patterns indicate an elevated risk that their injuries were caused by domestic violence, for instance, could be prioritized for a social worker visit in the ER. Interdisciplinary teams around the country like the Lutheran Settlement House Bilingual Domestic Violence Program in Philadelphia are thinking of other ways to support healthcare providers so that they can be more helpful to survivors. Of course, ultimately it is up to the survivor whether or not to disclose abuse, but at the very least survivors should have the best possible options for sharing their experiences and getting connected to help if they so choose.
While the value of connecting domestic violence survivors to services will only be as useful as the services are available and effective, we highlight system failures at an earlier step—determining who needs help in the first place. This is why the city of Chicago, in its new strategic plan to address gender-based violence, has joined institutions like the World Health Organization in pushing to strengthen data collection across sectors and expand where we can connect survivors to services, including in the health care system.
Authors






-
Acknowledgements and disclosures
The authors would like to thank University of Chicago trustee Emmanuel Roman for his financial support.
The Chicago Police Department had the right to review this publication to ensure no inadvertent confidentiality disclosures. Other than the aforementioned, the authors did not receive financial support from any firm or person for this article or from any firm or person with a financial or political interest in this article. The authors are not currently an officer, director, or board member of any organization with a financial or political interest in this article.
-
Footnotes
- If we look at injuries related to any form of inter-personal violence (whether domestic violence or some other type of assault or violent crime), among ER patients who had an X-ray about 50% more report violence victimization to law enforcement than to the ER medical staff. The police and the ER staff learn about only a partially overlapping set of violence incidents; the ER staff find out about only around a quarter of the violent victimizations the police learn about, while the police learn about just under half of the violence victimizations the ER staff learn about.
The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).



Commentary
Making the invisible epidemic visible
New approaches can help connect domestic violence survivors to services
August 16, 2023