Editor’s note: This post is adapted from a forthcoming full-length case study; the second in a series from the Engelberg Center’s Merkin Initiative on Physician Payment Reform and Clinical Leadership designed to support clinician leadership of health care delivery, payment, and financing reform. The case study will be presented during the Merkin Initiative’s
“MEDTalk” event
on July 9 from 10:30 AM to 12:30 PM EDT, featuring live story-telling and knowledge-sharing from patients, providers, and policymakers.
Oncology practices and hospitals across the nation struggle with providing sustainable, comprehensive, and coordinated cancer care. Clinical leaders with strategies and models to improve the quality and value of health care often don’t know how to navigate the landscape of payment and delivery reform options to sustain their innovations.
We use a case study approach to investigate and tell the story of the New Mexico Cancer Center (NMCC), an independent cancer center that is experimenting with innovative ways to improve patient-centered oncology care. We identify challenges for creating sustainable and supportive payments models, and we share the broader strategic and policy lessons for adopting alternative payment models.
The Clinical Scenario: Living With Cancer
Vicky Bolton, a 58-year-old full-time medical legal coordinator from Albuquerque, has stage 4 adenocarcinoma lung cancer. She started chemotherapy in 2003 and has consistently received treatments over the last 11 years. Vicky is one of 13 million Americans currently living with cancer, with more than 1.6 million new diagnoses added each year.
Although Vicky’s condition is currently stable, she is at high risk for venous thrombosis (blood clots), life-threatening infections, and other complications, which put her at high risk for repeated hospitalizations. In the past six months, she has taken advantage of “after hours” care on three occasions as an outpatient at NMCC. Fortunately, each of her providers and services — oncology, radiation therapy, labs, x-rays, and internal medicine — are centralized in a single location at NMCC, reducing the need for emergency room (ER) visits or hospitalizations for these episodes.
The Challenge: Controlling Spending While Improving Patient-Centered Care
Cancer is the second leading cause of death in the U.S. Forty-one percent of Americans will be diagnosed with cancer during their lives. Cancer care is also expensive, accounting for $125 billion of total health care spending annually. In 2011, Medicare alone spent nearly $35 billion in fee-for-service (FFS) payments for cancer care, representing 9 percent of all Medicare FFS payments.
The high costs of cancer care are driven by issues that plague the entire health system: uncoordinated care delivery, duplication of services, fragmentation, and volume-based payments. A common impact of these drivers in oncology is the use of the ER to relieve symptoms associated with adverse effects of chemotherapy or other treatments that can also result in hospitalization.
For example, research shows that the most common reasons for cancer patient ER admissions are pain, respiratory distress, nausea, and vomiting. More than half of the ER visits occurred on weekends or in the evening, and over 60 percent resulted in hospital admission. This suggests that if a patient’s symptoms could be managed at home or in the community, costly hospital admissions could be avoided. ER visits, where patients are exposed to germs and infections as they wait — often hours — to be admitted, can have catastrophic outcomes for patients that are actively in treatment since they have weakened immune systems and are more prone to infections.
In addition to the inherent issues with fee-for-service (FFS) payments — with payments incentivizing volume of procedures rather than the value of care delivered — the current payment system further exacerbates problems: If a practice provides higher-value care to patients at a lower cost to the overall system (that is, they perform fewer services and have lower revenue), the financial winner is the payer who reimburses fewer services, not the practice (which merely has less revenue). This combination of the misaligned incentives of FFS and the lack of financial benefit for improving care while reducing costs means that many practices simply cannot afford to make the transformations needed without other funding mechanisms.
The Real World: How Has An Independent Cancer Center Responded To These Challenges?
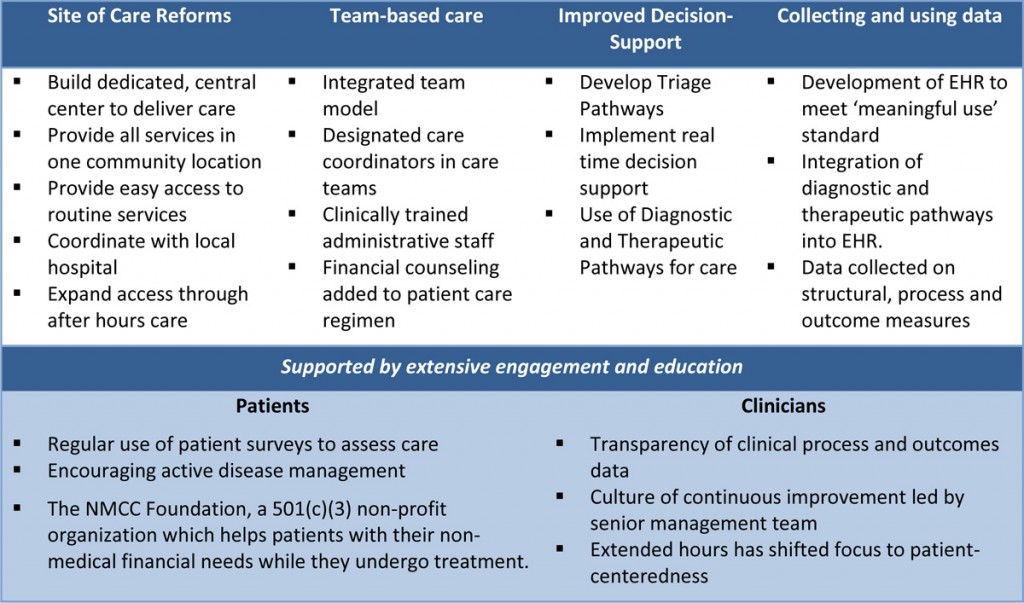
NMCC delivers care to roughly 2,700 patients and provides care to one in three New Mexicans with cancer. The changes that the center has made have focused on reducing the impact of fragmentation of care on their patients (Table 1).
A key innovation was enhancing comprehensive after-hours and weekend care on site and creating a telephone and urgent care triage program to avoid expensive emergency room and inpatient care, which NMCC termed the COME HOME model.
As part of its redesign process in 2012, NMCC – along with six community oncology practices — secured a $20 million Center for Medicare and Medicaid Innovation (CMMI) Health Care Innovation Award (HCIA), for a three-year period. The award has an explicit aim of reducing ER visits by 50 percent and hospitalizations by 20 percent to justify the program costs.
Table 1: Care Redesign Elements Undertaken by NMCC
The Key Levers: How Can COME HOME Be Sustained?
On the heels of the Affordable Care Act (ACA) and numerous quality and payment focused initiatives in the private sector, health care organizations need to enhance the competitiveness and efficiency of their systems in the marketplace.
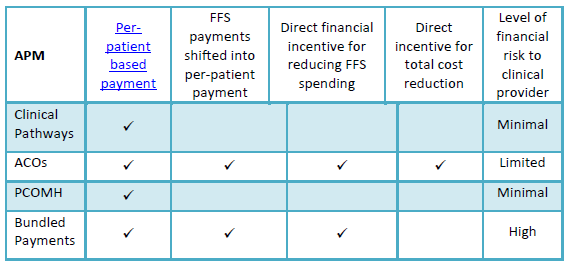
Alternative payment models (APMs) such as Accountable Care Organizations (ACOs), bundled payments, and patient-centered oncology medical homes (PCOMH) are just a few of the initiatives supported by public and private payers to align care redesign and payment reform and encourage continuous improvement. (Clinical pathways, a strategy recently embraced by WellPoint, offer PCOMH-like incentives to encourage adherence to practice guidelines, a strategy primarily geared to encourage higher-value chemotherapy practice.)
Broader or larger case-based payments may also provide stronger incentives to limit costs, to help assure that promising delivery reforms actually lead to cost reduction, but this exposes oncologists to greater levels of financial risk, as shown in Table 2. Consequently, implementing payment reforms that are viewed as feasible and desirable by both providers and payers is difficult.
Table 2: Comparison of Alternative Payment Models for Oncology
The Path Ahead: How Can These Models Assist NMCC?
NMCC currently receives approximately $70,000 per month from the CMMI grant and has not yet identified a clear strategy to sustain the delivery reforms in the COME HOME care model past the end of the grant (July 2015). As for payment reform options, NMCC has been unable to contract as part of a comprehensive ACO due to local health care market conditions.
Clinical pathways are geared primarily to guidelines and chemotherapy adherence, and are not designed to provide funding for after-hours care or triage programs that are intended to achieve offsetting savings through avoiding costly complications. Possible remaining options include:
- PCOMH: Using the data it gathers, NMCC intends to quantify the additional costs the COME HOME model requires, and the savings that it achieves. Based on that estimate, NMCC could suggest a per-member per-month (PMPM) payment from a private insurer to cover the costs of providing higher quality care. To encourage participation, NMCC could also enter into a risk-sharing agreement, in which overall costs of inpatient care and ER visits would be compared against a target. The PMPM payment could be at-risk if the targets are not achieved after a certain period of time.
- Bundled Payments: NMCC could potentially use the medical home approach with risk sharing (described above) as a first, interim step toward a bundled payment system, NMCC’s long-term preferred model. Computing actuarially sound expected costs for the bundled payments would require merging claims data with clinical data (for example, ICD-9 codes fail to distinguish between subtypes of breast cancer that have radically different treatments). A bundled payment pilot might be performed for high volume cancers, such as breast and lung.
Lessons Learned
The experience of innovative pioneers like NMCC can shed some light on potential barriers to conceptualizing and implementing sustainable clinical redesign. The lessons learned have been sorted into three main categories: relationships with payers and networks, payment model selection, and data collection and quality improvement considerations.
Relationships with payers and networks. Though counterintuitive, merely demonstrating significant value from care design, perhaps from lower utilization of inpatient and emergency department utilization, does not automatically create a financial pathway for sustainable delivery reform. To do so, innovative providers should consider involving lead payer partners early on to help identify end-points of interest to payers and potential payment strategies that may emerge later.
Providing support for health care delivery reforms requires new activities by payers towards aligning their payments with value, rather than volume and intensity of services. However, fragmented health care markets face the challenge of the “free rider” problem: payers may be unwilling to shoulder delivery transformation costs that may benefit other payers’ clients while they wait for CMS or others to make the financial investment, pay for the program evaluation, and enact policy change). Other challenges include payer inertia and long lag times between care redesign and subsequent data demonstrating results.
Large ACOs and other integrated payer-provider plans, including those large enough to form Medicare Advantage plans, are moving forward on negotiating payment and delivery reforms. This may be more difficult for innovative, smaller practices, even if they can provide higher-value clinical services. In turn, this may have anti-competitive consequences, such as discouraging delivery innovation that leads to “demand destruction” of high-cost hospital-based services. Private and public payers should be particularly interested in developing models that enable smaller, specialized providers like oncology practices to undertake key delivery reforms.
Sustainable Payment Model Selection. While substantial attention has been paid to primary care focused APMs, specialty-focused APMs are needed for practices like NMCC. Their development should be a high priority for public and private payers. Clinical transformation grants, such as those offered by CMMI, should include clear pathways for transitioning to APMs if initial cost savings targets or projections are met. Otherwise, delivery system innovations are at high risk of failure despite evidence of improved value.
Data Collection and Quality Improvement Considerations. Timely sharing of actionable information from claims and other administrative data remains a major challenge, with complex and varied procedures for obtaining claims from payers; smaller practices are particularly challenged in interpreting the claims data. Some states, such as Maryland, Massachusetts, Vermont, and Colorado (among others) are proceeding with creating all-payer claims databases. (Maryland, for example, offers almost instantaneous provider feedback from claims through their CRISP database.)
Others, such as Minnesota, are using “distributed” approaches in which multiple payers and systems produce measures in consistent ways. As NMCC’s early efforts illustrate, practices can produce more clinically sophisticated performance measures. Strategies to achieve consistent methods for sharing key data on cost and quality need to be expanded to encourage quality improvement and payment reform.
The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).



Commentary
Op-edPayment and Delivery Reform Case Study: Cancer Care
July 7, 2014