What’s the latest in health policy research? The Essential Scan, produced by the Schaeffer Initiative for Innovation in Health Policy, aims to help keep you informed on the latest research and what it means for policymakers. If you’d like to receive the biweekly Essential Scan by email, you can sign up here.
Medicare Advantage physician payments roughly equal to traditional Medicare; rates for lab services and medical devices lower and more akin to commercial rates
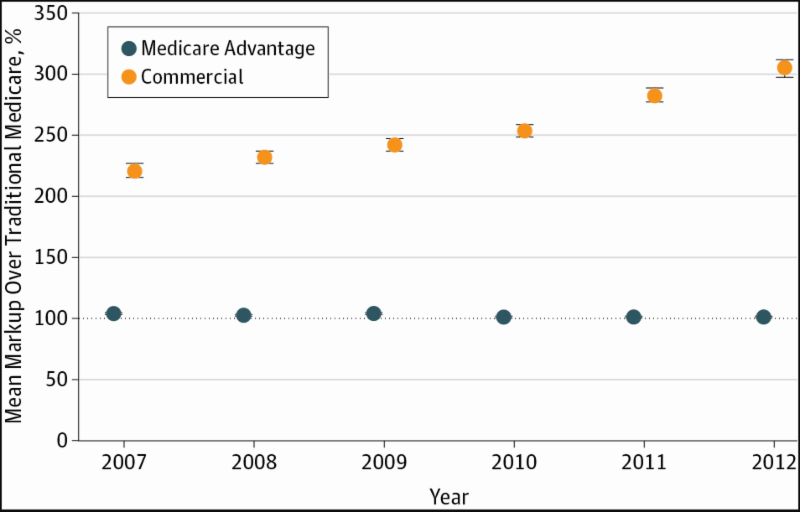
Erin Trish, Paul Ginsburg, Laura Gascue, and Geoffrey Joyce find that the average reimbursements by one Medicare Advantage (MA) insurer range from 91.3 to 102.3 percent of traditional Medicare for physician services, in most cases, substantially lower than rates for commercial plans. But when commercial prices are much lower for services, such as for lab services and durable medical equipment, MA plans follow commercial pricing, with reimbursements for lab services and equipment ranging from 67.4 to 75.8 percent of traditional Medicare rates. Using claims data from 2007 to 2012 from one insurer with both a significant MA and commercial presence, these findings raise questions about whether MA plans would have to pay higher rates if traditional Medicare no longer was an option, such as in some premium support proposals, and suggests that Medicare is paying too much for lab services and durable medical equipment. Full article here.
Low levels of competition in generic drug market lead to higher prices
Chintan V. Dave, Aaron S. Kesselheim, Erin Fox, and co-authors find that increases in generic drug prices were strongly associated with low baseline levels of market competition. While the median price for generic drugs in their sample decreased by 16.3 percent during the study period (2008 to 2013), drugs in monopolistic or near-monopolistic markets saw price increases of 47.4 percent and 20.1 percent, respectively. Meanwhile, drugs in duopolistic and quadropolistic markets saw prices decrease by 11.8 percent and 31.7 percent, respectively. Of the 1120 drugs examined, almost half were in duopolistic markets. Low levels of market competition affected the prices of lower priced drugs more than higher priced drugs and changes in market competition during the study period did not have a strong effect on drug prices. The authors outline several potential reasons why market forces fail to regulate overpriced generic drugs such as lack of awareness of drug price changes caused by the small size of the markets for some generic drugs or an inability to quickly scale up manufacturing. Full article here.
Post-acute care potential source of waste in US healthcare system
Joseph J. Doyle Jr., John A. Graves, and Jonathan Gruber exploit the near random assignment of similar patients to different hospitals by ambulance companies to identify post-acute care rendered at skilled nursing facilities (SNF) as a potential source of waste in the US healthcare system. Using Medicare claims data from 2001 to 2012, the authors find that patients who are sent to hospitals with higher total spending (inpatient and downstream) only had 2 percent lower mortality rates compared to patients sent to lower spending hospitals. The authors find that inpatient expenditures were associated with better health outcomes while higher downstream spending through post-acute SNF care was associated with higher mortality rates. These findings suggest that post-acute SNF admissions could serve as a measure of quality in future hospital evaluations. Full article here.
Consumer-directed health plans not associated with a decrease in preventive screenings
Matthew D. Eisenberg, Amelia M. Haviland, Ateev Mehrotra, Peter J. Huckfeldt, and Neeraj Sood find that being offered or enrolling in a “consumer-directed” health plan (CDHP) did not affect cancer screening rates in the three years following enrollment in the plan. CDHP enrollees did, however, increase screenings in the final three months before switching plans, demonstrating a possible poor understanding of CDHP benefit design. The authors posit the extended time horizon of the study may have captured enrollees learning that preventative care screenings are not subject to cost-sharing under these plans as well as an initial “stockpiling” of services prior to switching, underlying the importance of studying effects over the longer-term. These findings add to the body of research about the effect of CDHP enrollment on preventative care use. Full article here.
Indication-based pricing for pharmaceutical drugs lead to higher prices
Amitabh Chandra and Craig Garthwaite argue that “indication-based” pricing for pharmaceutical drugs-which relies on identifying specific biomarkers to gain insight into the true value of a particular drug for a specific consumer-is akin to price discrimination and would negatively impact many consumers. While advocates for indication-based pricing argue that it would lower costs for the majority of users without harming those who need the drugs most, Chandra and Garthwaite warn that such a pricing scheme would allow pharmaceutical companies to extract the maximum amount of money from each patient, which would in turn lead to higher drug prices or more limited access for those who value a drug the most and increase utilization for those who value a drug the least. They argue these competing effects would lead to higher overall spending and higher manufacturer profits relative to uniform pricing. Full article here.
Related Content


Authors



The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).



Commentary
The essential scan: Top findings in health policy research
July 25, 2017