
Introduction
For many children with chronic conditions, daily routines coordinated by parents and caregivers are a critical part of treatment. In a new study, we show that when those routines were disrupted with the onset of the COVID-19 pandemic, adherence to asthma control medication declined substantially. Drawing on national pharmacy claims data covering nearly all U.S. prescriptions, we find that children’s use of these medications declined sharply during the first year of the pandemic—especially for the youngest patients. By December 2020, adherence among preschool-aged children was down roughly 40% compared with 2019. Adults, by contrast, increased adherence to their own medications, underscoring that the decline was concentrated among children with asthma rather than a general fall in medication use.
These patterns point to a distinct vulnerability in pediatric health care: Treatment for chronic conditions often depends on family schedules and attention that can be easily disrupted. The declines that we find were widespread across the country and intensified beyond the early lockdown period, suggesting a sustained breakdown in medication routines rather than a short-term access problem. The prolonged decline is also inconsistent with a change in medical need, such as fewer asthma triggers early in the pandemic, because these factors would have diminished as daily activities resumed.
These findings underscore a broader lesson. Pediatric health care systems that rely on continuous effort from families are fragile. Simple design choices such as longer prescription supplies, automatic refills, or synchronized family pickup schedules can help make pediatric care more resilient to everyday and large-scale disruptions alike.
Children’s medication adherence was fragile long before the pandemic
Children with chronic conditions like asthma depend on regular, sustained treatment to prevent symptoms and avoid emergency care. For controller medications—medications taken routinely to manage baseline symptoms—success requires that prescriptions are filled on time so that medication is available consistently. In practice, these steps rely on parents and caregivers to maintain schedules, request refills, and build medication use into daily life. When these routines are disrupted, adherence can fall—even when medications are affordable, effective, and available.
Before the pandemic, our data show that medication adherence among children was already low relative to adults with comparable prescriptions. In 2019, children with chronic asthma had controller medications available on fewer than half of days in a typical month—well below the 50% threshold often linked to poor long-term control and higher health care use. Several sudies document parents’ central role in managing pediatric medication routines. This evidence underscores that children typically begin from a lower baseline of adherence than adults, in part because effective treatment depends on the sustained involvement of caregivers.
This dependence makes pediatric health care uniquely sensitive to disruptions in daily life—a sensitivity that was likely amplified during the pandemic. In normal times, families must manage treatment around school schedules, work hours, transportation, and competing caregiving demands. National survey data from the RAPID-EC project show that in 2020, parents of young children reported sharp increases in stress, caregiving burden, and financial strain. As family stress rose and daily routines were disrupted, children’s medication use faltered. The resulting declines in adherence are not only indicators of lost stability within households but also signals of structural weakness in how the health system supports chronic pediatric care.
Asthma is one of the most common chronic pediatric health conditions and a leading cause of pediatric hospital visits and missed school days. Because symptoms and management are closely tied to family resources, disruptions in adherence can reinforce broader inequities in child health. Studies show that socioeconomic differences in children’s early health translate into lasting gaps in education attainment and adult well-being. Low adherence to controller medication therefore matters not only for short-term asthma control but also as part of the accumulation of disadvantage over time. Strengthening the systems that help caregivers manage chronic pediatric conditions is thus an investment in both immediate and long-term health equity.
Nationwide prescription data reveal how routines broke down during the pandemic
Our analysis draws on a near-universe of U.S. prescription claims between 2018 and 2020, covering roughly two million pediatric asthma patients per month. Individuals were included in our analysis if they had at least one controller medication fill between January and March of each year, and we then track their prescription activity through December. About 60% of pediatric patients in our analysis are male, and they are, on average, 9 years old. They are concentrated in areas with an average per-capita income of about $32,000, where roughly one-quarter of residents are members of minority groups, one-fifth have some college education, and nearly 90% live in urban areas.
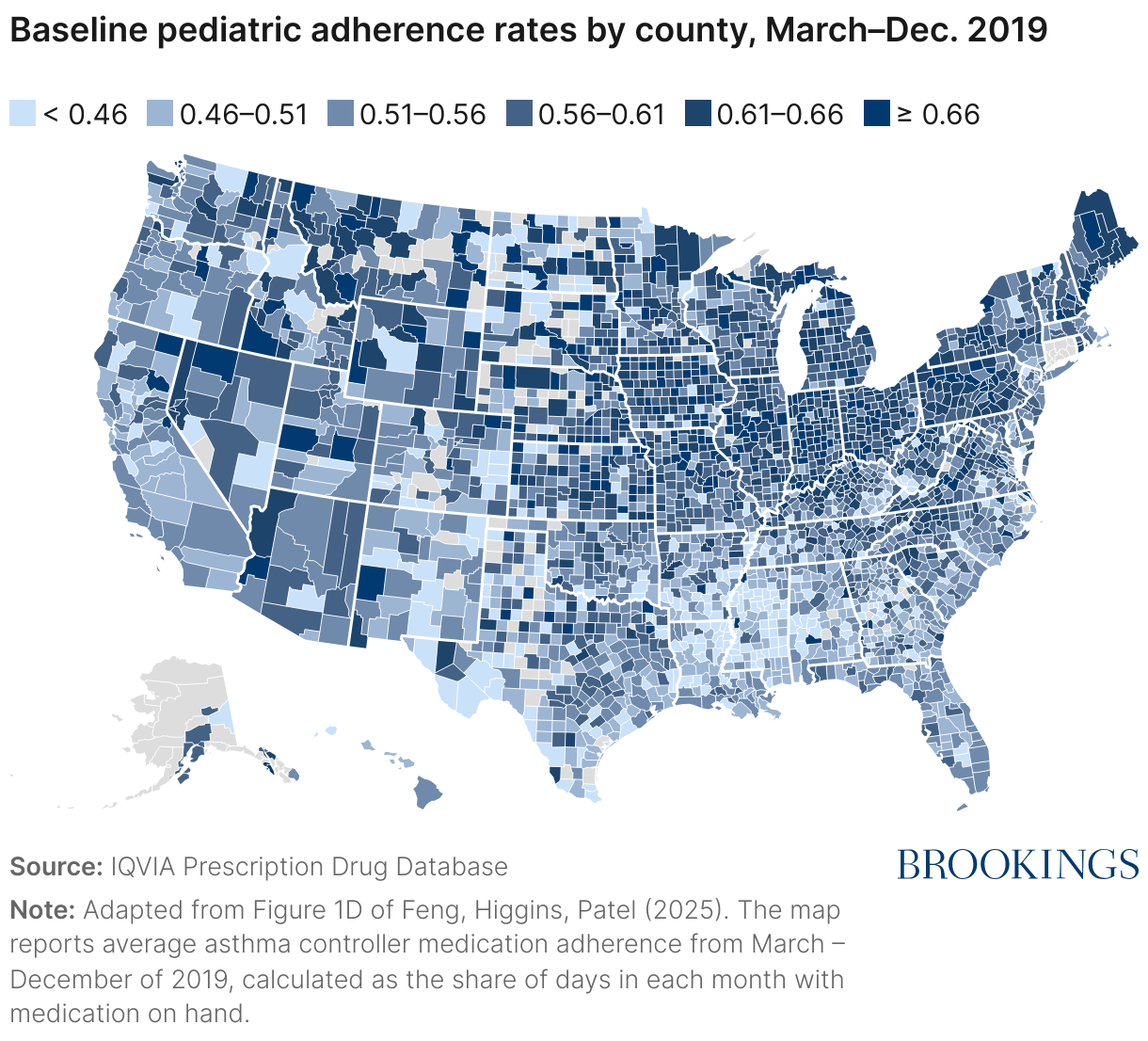
Figure 1 shows adherence rates—measured as the proportion of days covered by asthma controller medication—in 2019 for these patients from March through December. The figure maps the share of days in each month in which patients had controller medication available, averaged across these ten months. Adherence varied widely by geography, with lower adherence rates more concentrated in the South and Mountain West. These pre-pandemic patterns establish a baseline against which to measure 2020 changes
During 2020, adherence plunged, especially for the youngest children
We find that adherence to asthma controller medications among children fell sharply with the onset of the pandemic. Comparing each month of 2020 with the same month in 2019, average adherence dropped by roughly 13% from March through December. Declines were steep both in the early months of the pandemic and again at the end of the year, suggesting both that adherence did not rebound as daily life adjusted to the pandemic and that the disruption to medication routines was prolonged.
We also find especially large effects for younger children. By December 2020, adherence among preschool-aged patients was roughly 40% below its 2019 level, compared with declines of about 25% for school-aged children and 21% for adolescents. These large declines among the youngest children are particularly concerning because they are the least able to recognize symptoms, communicate their needs, or manage medications without direct caregiver support.
As shown in Figure 2, declines were also widespread across the country. Most counties experienced substantial reductions in adherence. The consistency of the pattern across regions and income levels underscores that these declines reflected a national disruption in children’s medication routines rather than local access problems or supply constraints.
![[ Insert title here ] (Choropleth map)](https://datawrapper.dwcdn.net/Nk3nC/full.png)
Adults, by contrast, increased adherence to their own medications during this period, reinforcing that the downturn among children was specific to pediatric care and not a system-wide change in prescription behavior.
Disrupted family routines, not access or need, most likely drove the decline
The patterns that we find point to attention and household routine as the main drivers of the 2020 decline rather than access, supply, or a change in need. Although asthma triggers such as physical activity and respiratory illness may have fallen early in the pandemic, those reductions cannot explain the large, persistent, and age-skewed declines that we observe.
Two pieces of evidence support this interpretation:
- First, children whose parents used mail-order pharmacies before the pandemic—an arrangement that simplifies refills and reduces travel burdens—experienced smaller drops in adherence. Specifically, we estimated that pre-existing mail-order use offset about 40% of the average decline between August and December.
- Second, children’s adherence fell less in families where adults were filling their own prescriptions, suggesting that parental medication routines help sustain children’s treatment.
Other pandemic-specific factors such as school closures, telehealth expansion, changes in air quality, and local insurance coverage were only weakly related to the size of the decline once age and mail-order use were considered. Together, these findings point to a clear policy challenge: making children’s medical care less dependent on daily family routines and more resilient to disruption.
Making pediatric care more resilient
The pandemic revealed how strongly pediatric care depends on parental and caregiver attention and how small design choices can make that dependence more manageable. Policymakers, insurers, providers, and families all have roles to play in strengthening these routines and reducing the attention required to maintain treatment.
- Simplify adherence: Insurance providers and pharmacies can make long-term controller use less attention-intensive by defaulting to 60- or 90-day supplies, enabling automatic refills, and making mail delivery simple to opt into.
- Coordinate across family members: Plans can let families align refill dates across prescriptions, and pharmacies can offer synchronized pickup or delivery schedules. Because many medications are filled on fixed cycles (i.e., 30 days), even small timing differences between family members’ prescriptions can leave refills days apart. State insurance regulators could encourage this by establishing family-centered pharmacy standards.
- Support routine building in care settings: Pediatricians, pharmacists, and schools can reinforce consistent medication use by sending refill reminders, discussing refills during visits, and coordinating with families on intensive maintenance regimes.
- Target support for the youngest children: Because adherence gaps are largest for the youngest patients, outreach and benefits design could focus on families with pre-school- and elementary-aged children. For example, medication management reminders could be integrated into WIC, Head Start, or early-childhood health programs.
These steps would make adherence more resilient to the disruptions that families inevitably face. Strengthening the infrastructure that helps children stay on treatment is not only good health policy—it’s an investment in long-run health and equity that can be especially impactful when families face financial or personal stress.
Authors


The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).


