This analysis is part of the USC-Brookings Schaeffer Initiative for Health Policy, which is a partnership between Economic Studies at Brookings and the University of Southern California Schaeffer Center for Health Policy & Economics. The Initiative aims to inform the national health care debate with rigorous, evidence-based analysis leading to practical recommendations using the collaborative strengths of USC and Brookings.
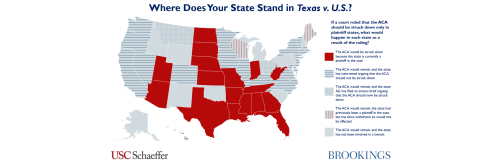
Last month, the Fifth Circuit reached a decision, of sorts, in Texas v U.S., the lawsuit in which the Trump Administration has joined Texas and several other states in arguing that the entire Affordable Care Act should be invalidated. The Fifth Circuit held that the law’s individual mandate is now unconstitutional, since Congress reduced the penalty for violating the mandate to $0. However, on the most critical question of the case – what other parts of the ACA should be invalidated on the grounds that they are inseverable from the mandate – the court essentially punted, remanding the case back to the district court for additional analysis. Further, in remanding the case to the lower court, the Fifth Circuit expressed a clear openness to the arguments made by Texas and the Trump Administration that the entire ACA, not just the provisions related to reform of the insurance market, should be struck down.
There is little basis in the relevant body of law for this remand. As the dissenting judge in the Fifth Circuit and nearly all legal experts have noted, the severability questions presented by the case are straightforward, and the appeals court ought to have easily reached the conclusion that the ACA should remain in force. Further, the lower court judge who will hear the case on remand has already held – in December of 2018 – that the entire ACA must be struck down, and few observers expect a different outcome here. But the additional analysis the Fifth Circuit requested could take months or even years. Thus, additional proceedings in the lower court will serve only to delay reaching a final decision in this case, almost certainly by the Supreme Court.
The extended period of uncertainty is unnecessary and will impact stakeholders across the health care industry. Moreover, while some uncertainty may have existed since the lawsuit was first filed or since the lower court judge reached a decision in late 2018, the Fifth Circuit’s seeming openness to the argument that the entire law should be invalidated, combined with the Trump Department of Justice embracing that view in early 2019, has increased the stakes.
This blog considers some of the specific policy consequences of uncertainty in segments of the health care market.
Consumers with pre-existing conditions
Perhaps the most widespread harms will be experienced by consumers with pre-existing conditions. Analysis indicates that between 27 and 50 percent of adults have a pre-existing condition that could affect their ability to obtain health insurance in the individual market if the ACA was invalidated. Many of those consumers today receive health insurance from their employer and are not directly impacted by the ACA’s prohibition against discrimination based on health status in the individual insurance market or the financial assistance the law provides to help people afford coverage. Yet each time someone who has job-based health insurance considers a change in their employment status or faces the loss of their job they can, under current law, expect that they will have a way to obtain insurance if they were to lose their employer coverage.
An extended period of judicially-created uncertainty about the future of the law could erode that reliance. Instead, when the many tens of millions of Americans with pre-existing conditions are making decisions about retiring early, working part-time, changing jobs, or starting a new business, they may feel compelled to consider how the absence of the ACA’s protections would affect their decision. Some people may ultimately opt to postpone retirement or forego starting a new business amid that uncertainty, foregoing benefits that would accrue to them and their community if they had not been forced to make a decision amid uncertainty. And some who rely on the ACA for coverage today may be induced to seek employment with group health insurance to protect themselves against future changes, making suboptimal decisions to preserve their access to coverage. For any given consumer the impact of uncertainty may be small, but millions of people remain potentially affected.
Health care providers
The financial interests of the vast majority of American health care providers are impacted by the ACA. The law affects providers in two primary ways: (1) it dramatically reduced the uninsured rate, creating a larger pool of customers and reducing uncompensated care, and (2) it directly affects provider payment by changing some Medicare and Medicaid payment rules and creating new payment models. Undoing these policy changes by invalidating the ACA would have widespread impacts on providers. Therefore, providers facing uncertainty about the future of the ACA may make different investment decisions than in a settled policy environment.
As just one example, in Arkansas, repeal of the ACA would be expected to increase the uninsured rate from 8% to 20%. The available evidence suggests this impact would be concentrated in rural areas, and that the ACA’s coverage gains have had a particularly large effect on coverage for substance use disorder services. A rural health system in Arkansas might be considering whether to invest in expanded capacity to treat individuals with substance use disorder, especially in light of the prevalence of opioid use in the state. But the potential for the overall uninsured rate to more than double – wiping out coverage for substance use disorder services for many potential patients – may complicate the system’s decision-making around that investment. Thus, extended uncertainty about the future of coverage could ultimately delay needed investments in health care infrastructure, with the greatest risks falling on vulnerable communities who are most likely to be impacted if the ACA is invalidated.
Related Books


Engagement with the new payment models under the ACA might also be delayed. Some of the ACA’s payment changes are mandatory and some are voluntary for providers. The voluntary models have the potential to save the federal government money by reducing the total cost of care provided. Today 10.9 million Medicare beneficiaries receive care from a provider participating in the Medicare Shared Savings Program, and many more receive care from providers participating in other arrangements. However, it only makes sense for a provider to commit to a voluntary payment model if they make investments to change how care is delivered. This can include a hospital developing new relationships with community-based service providers or groups of doctors coordinating care delivery with one another – processes that often require a large upfront commitment of time, training, and technology investments. But if the ACA is invalidated, the federal government will no longer be able to uphold its end of the bargain, leading to wasted investment. The uncertainty could delay uptake of voluntary payment reforms, particularly among providers who are otherwise unsure about whether to commit to the practice changes required.
In addition, providers facing mandatory payment reforms might also face a complicated set of choices. For example, if the federal government were ever to move forward with a proposed mandatory change to the way it pays for radiation oncology that is authorized by the ACA, affected providers would need to decide whether to make the necessary changes to maximize revenue under the new payment system, or continue their old practices, which might lead to some short-term revenue loss but would leave them better positioned if the ACA (and therefore the payment change) were invalidated. This decision is further complicated by the fact that the federal government proposing the new mandatory model is simultaneously arguing in Texas v. U.S. that its authority to implement the model should be invalidated – making it difficult to determine their commitment to pursuing these changes.
State governments
The ACA represents a major new investment of federal resources in state budgets. In some states expanding Medicaid, the law represents a nearly 40% increase in federal fund inflows (from all sources) to the state government. The spending facilitated by the law has been associated with, of course, large coverage gains as well as more stability in health systems and job creation within and outside the health care sector. Moreover, the law’s Medicaid expansion can lead to reductions in state spending on public health, behavioral health services, and uncompensated care. Funding provided by the law has clearly become a major component in state spending. The potential loss of a significant fraction of federal funding is a cloud of uncertainty that could affect a wide variety of state investments.
Pharmaceutical companies
Harms to consumers, providers, and states are widespread and could affect dozens of overlapping decisions, reflecting the fact that the ACA changed so much about the health care system. Conversely, there is one group of stakeholders that may experience an extremely concentrated problem of uncertainty: manufacturers of biosimilar drugs.
Biosimilar drugs are the “generic” version of biologic drugs (which are a chemically complex and costly form of specialty drugs). Prior to enactment of the ACA, there was no pathway for the FDA to approve a biosimilar drug; a proposed biosimilar would need to go through a full, expensive approval process as if it were a new biologic. The ACA authorized the FDA to approve biosimilars through a more appropriately scaled process. But invalidating the ACA would strip the FDA of that authority, making it unlawful for them to approve any new biosimilar drug.
What, then, is a biosimilar manufacturer to do? Should they continue the research and development necessary to seek approval of new biosimilar drugs, which could save the health care system billions of dollars but requires an upfront investment of tens or hundreds of millions of dollars over several years? Or should they forego new biosimilar research until there is greater certainty about whether it will remain lawful to sell the product? Drug manufacturers face tremendous scientific uncertainty and already must make investments with unknown payoffs; compounding this with judicially-created uncertainty could lead to reduced investment in cost-saving biosimilar drugs, at least at the margin, for as long as this litigation persists.
*****
Other stakeholders – including insurance companies, the Indian Health Service, and high-income taxpayers – are affected by the ACA and therefore face potential uncertainty. Certainly, for everyone affected by the law, a number of factors, including how stakeholders weigh the likelihood of a decision striking down the ACA and how central the ACA is to a decision or business model, will affect the ultimate magnitude of the consequences of judicially-created uncertainty. Stakeholders may also attempt to predict the likelihood of Congressional action in the event that the ACA is ultimately invalidated, particularly in the less controversial policy areas, and that may blunt some of the impact. Nonetheless, these types of harms are a byproduct of the delay that the Fifth Circuit’s remand will cause.
Related Content

Author

The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).



Commentary
Remanding Texas v. U.S. to the lower court prolongs harms to consumers and the health care industry
January 3, 2020