This report was amended on January 22, 2026 to provide additional clarity about which actions were taken under the Regional Transportation Optimization initiative.
Introduction
Mail-order pharmacies are a cornerstone of the nation’s prescription delivery network, particularly for chronic conditions that require consistent access to medication. By eliminating travel barriers and providing longer-fill prescriptions—usually 60- or 90-day supplies rather than the typical 30—mail order supports regular treatment routines that are central to chronic-disease management. The value of mail-order prescriptions links the performance of the postal network directly to the continuity of pharmaceutical care, making changes in speed or reliability of the postal network a serious health care issue, not just an inconvenience to post office customers.
In recent years, the United States Postal Service’s (USPS) has launched its Delivering for America (DFA) strategic plan to modernize its network and reduce costs. Key elements of this consolidate mail processing into regional hubs and reduce the frequency of mail pickups for certain post offices. While intended to improve efficiency, early analysis by oversight bodies like the Postal Regulatory Commission warns that delivery slowdowns may be unevenly distributed, particularly in rural areas where dependence on mail-order pharmacies is highest.
Using near-universal prescription transaction data for asthma and diabetes medication in 2019, this report maps where and for whom mail-order medication is most prominent. Combining these data with measures of pharmacy access, postal infrastructure, and and exposure to structural/operational changes under the DFA identifies where multiple vulnerabilities overlap. Roughly 3.7 million Medicare-eligible Americans live in communities where three risks to medication access converge: limited retail pharmacy access, heavy reliance on mail-order prescriptions, and exposure to postal service restructuring. In these largely rural areas, even small changes in mail speed or reliability can interrupt medication schedules and undermine the management of chronic disease.
The resulting “triple burden” analysis illustrates how the postal system functions as a critical—if often overlooked—component of the nation’s health infrastructure, and how operational changes designed for efficiency may carry unintended health consequences.
Understanding the operational changes and geographic impact of the Regional Transportation Optimization
The Delivering for America (DFA) plan, introduced in 2021, outlines the U.S. Postal Service’s 10-year strategy to modernize operations and restore long-term financial stability. The plan emerged after years of operating losses driven by declining mail volumes and the broader shift towards digital communication. One of the plan’s core objectives is to reduce costs and improve efficiency across the delivery network while maintaining universal service coverage. The Regional Transportation Optimization (RTO), rolled out in 2024, is a key part of this effort.
Mail that was once processed locally is now transported to larger regional facilities for processing. Many local post offices—especially those located more than 50 miles from a regional processing center—are moving to a single daily collection schedule for outgoing mail under the RTO. Because dispatches to these regional processing facilities now only occur once per day, the change slows the movement of mail, effectively extending end-to-end delivery times in affected communities.
The Postal Service describes this shift as part of a broader effort to enhance service reliability and efficiency by consolidating transportation routes and aligning network operations with current mail and package volumes. In this view, modestly slower delivery is intended as a trade-off for a more predictable and financially sustainable network. Oversight bodies, however, have questioned whether the expected reliability gains are materializing. The Postal Regulatory Commission (PRC) concluded in its 2025 Advisory Opinion that the plan could bring a “certain downgrade in service for a significant portion of the nation,” noting a “considerable decline in service performance has already been demonstrated in areas such as Richmond, Virginia, and Atlanta, Georgia, where proposed network changes have already been implemented. Similarly, the Postal Service’s own Office of the Inspector General has found that “early implementation of this transformation have resulted in negative service impacts,” with on-time delivery rates for First-Class and Priority Mail decreasing despite the new standards. Together, these findings suggest that while the changes seek to improve operational consistency, its near-term effect has been slower and, in some regions, less reliable service.
These recent operational changes build on a service environment that has already slowed. In 2021, USPS formally extended the expected delivery window for much of First-Class Mail from one-to-three days to three-to-five days as part of the DFA implementation. The RTO rollout does not change these published standards but may further extend actual delivery times in areas farther from processing centers, particularly where the new 50-mile threshold requires additional surface transport before sorting and dispatch.
The PRC’s broader 2025 Advisory Opinion echoes these concerns, emphasizing that the network changes are likely to have uneven geographic effects. It described USPS’s projected cost-savings estimates as uncertain and expressed concern about “the disproportionate impact that the proposed changes will have on rural communities across America,” where greater distances to processing centers may make it more difficult to meet existing delivery standards.
These changes raise spatial equity concerns because they introduce systematic geographic variation into what has historically been a universal public service. Those served by post offices that are located farther from RPDCs are more likely to experience slower collection and longer delivery cycles, compounding existing disparities in access to time-sensitive goods and communications. Figure 1 maps the share of each county’s population that is served by a post office that is affected by the RTO. This exposure is estimated by measuring the distance from the centroid of each census block to the nearest post office, and then block exposures are aggregated to the county level using population weights. Exposure to the RTO is highest in rural and low-density regions, where longer travel distances between communities and processing centers make the restructuring the most consequential.
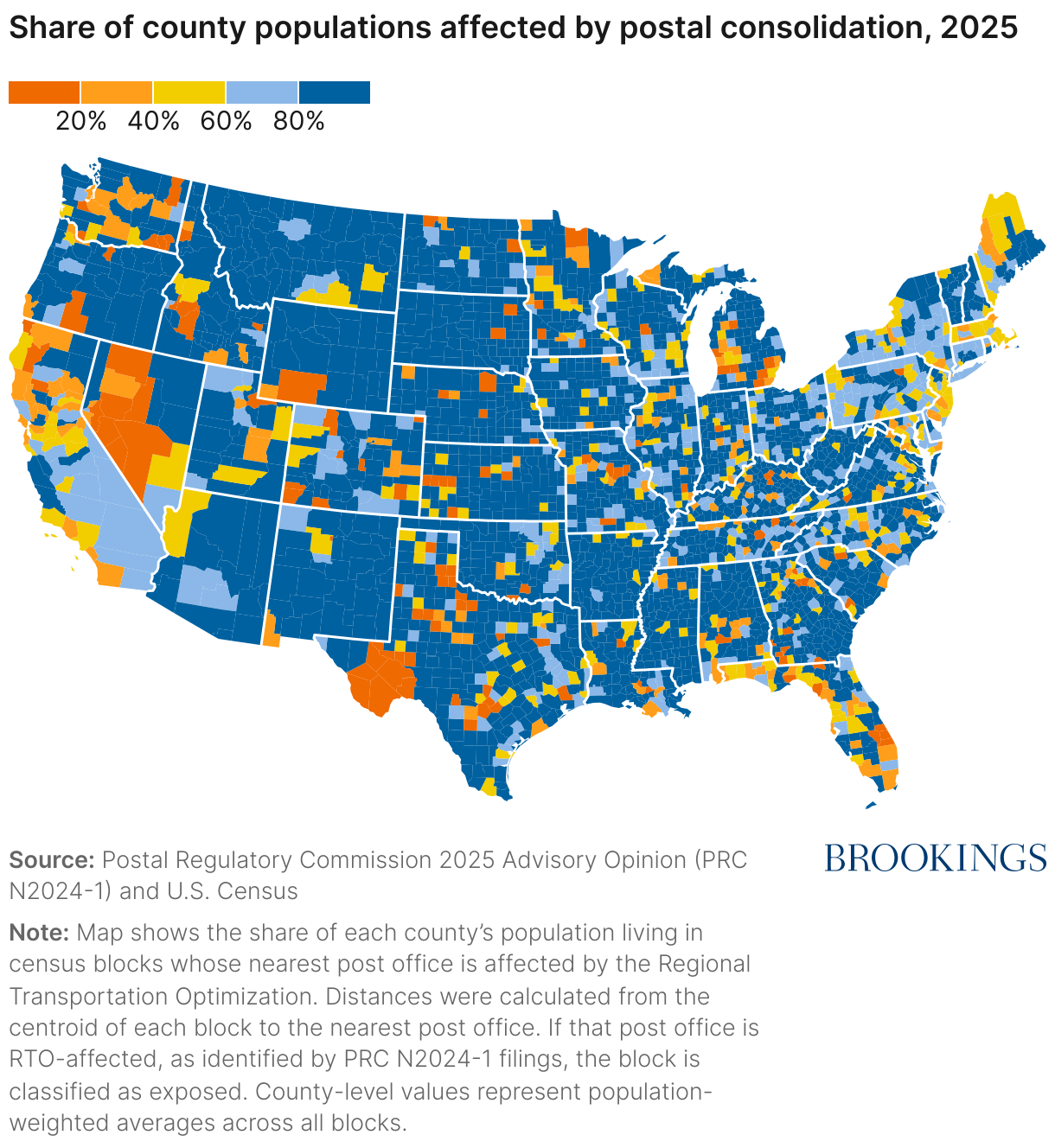
While USPS modernization aims to improve the efficiency and sustainability of the postal network, the geography of the RTO implementation shows that the costs of the adjustment are not evenly distributed. Households located in less dense areas are farther from regional processing centers and face a higher likelihood of slower or less predictable mail. These conditions have practical implications for households that rely on the mail for essential goods. These effects are especially likely to be evident in the delivery of prescription medications, where mail-order fulfillment has become an important channel for maintaining consistent access to care.
Mail-order medication patterns for chronic conditions
Mail-order medication and health outcomes
Medication adherence is a central determinant of health outcomes for chronic conditions like asthma and diabetes. When patients fail to take medications as prescribed, rates of hospitalization increase, raising both individual and system-level costs. Logistical frictions reduce adherence; for this reason, delivery channels that lower the effort required to fill and maintain prescription supplies have become important determinants of adherence.
Mail-order pharmacies can alleviate many of these barriers by offering longer refill periods, automated refills, and home delivery that eliminates travel and wait-time costs. A systematic review of adherence among mail-order versus retail dispensing consistently found higher adherence among mail-order users across multiple disease classes (Fernandez et al. 2016). Similarly, large administrative data analysis of home-delivery programs shows 30-40% fewer non-adherent patients relative to retail channels. Experimental evidence from an integrated health care system further confirms that encouraging mail-order uptake improves adherence outcomes.
Evidence from recent adherence research reinforces these findings. New evidence from national prescription claims shows that pre-pandemic mail-order use buffered against declines in pediatric asthma control during COVID-19 disruptions. Complementary research demonstrates that pharmacy access itself influences medication use: Pharmacy closures reduce short-term drug consumption, especially among low-income and rural Medicare patients, underscoring how delivery channels and local dispensing capacity jointly shapes adherence and health outcomes.
Taken together, these findings point to a central implication: The benefits of mail-order medication are related to timely, predictable delivery. These conditions directly connect postal network performance to medication adherence in the population.
Nationwide prescription drug transactions: IQVIA
This analysis draws on comprehensive prescription transaction data from IQVIA, covering nearly all retail and mail-order pharmacy claims in the U.S. for asthma and diabetes medications during 2019. Focusing on a single pre-pandemic year provides a baseline view of medication access that predates the DFA and subsequent RTO restructuring. This offers a benchmark for understanding patterns of mail-order use before major postal network changes.
Asthma and diabetes are among the most common and costly chronic conditions in the U.S. and are widely studied in the context of medication adherence. Both require ongoing pharmacological management to control symptoms and prevent severe health events, and their treatments—ranging from maintenance inhalers to oral therapies—are readily dispensed through mail-order channels. These conditions span age groups, insurance types, and geographic settings, making them robust indicators of how speed and reliability relate to chronic-disease management across the population.
The IQVIA database records each prescription fill with information on the dispensed drug, fill date, days supplied, delivery channel (mail-order or retail), payer, and the zip code of the prescribing provider. The dataset captures dispensing for virtually all payers including commercial insurance, Medicare, Medicaid, and cash transactions, making it one of the few data sources capable of describing the complete landscape of medication distribution across the U.S.
Data caveats: IQVIA prescription claims data offer extensive national coverage but are not fully universal across all dispensing channels. IQVIA reports that its longitudinal prescription database captures over 90% of retail transactions and approximately 85% of all mail-order prescription claims. As a result, estimates of mail-order utilization may modestly understate true volumes, particularly in markets dominated by specialized or vertically integrated mail-service providers. In addition, payer-type classifications are not fully separable. Medicaid managed care plans are grouped with commercial managed-care plans; fee-for-service Medicaid is separately identifiable, but these plans cover a small share of Medicaid populations in 2019.
Baseline patterns of mail-order medication use
Mail-order use is measured as the share of total prescriptions filled for either asthma or diabetes medications dispensed through mail-order channels rather than at retail-pharmacies. Table 1 summarizes tract-level prescription patterns for asthma and diabetes medications. For each tract, this share is calculated across all prescriptions filled in 2019. A census tract represents a small, relatively uniform geographic area defined by the U.S. Census Bureau, typically containing about 4,000 residents. Zip-code level data are mapped to tract and county boundaries using population-weighted crosswalks maintained by the Department of Housing and Urban Development (HUD), allowing prescription patterns to align with demographic and postal infrastructure data.
|
Asthma |
Diabetes |
||||||
|---|---|---|---|---|---|---|---|
|
Mean |
Std Dev |
Median |
Mean |
Std Dev |
Median |
||
| Prescriptions per tract | 1,330 | 1,970 | 818 | 1,608 | 2,270 | 1,038 | |
| Share mail-order | 4.2 | 3.3 | 3.9 | 6.4 | 3.8 | 6.1 | |
| Days Supplied | 35.5 | 4.7 | 35.5 | 50.2 | 6.2 | 50.2 | |
| Share Medicare | 24.9 | 9.5 | 24.5 | 34.7 | 9.3 | 34.6 | |
| Share Third-Party (inc. Medicaid MCO) | 67.5 | 14.0 | 70.1 | 58.4 | 10.8 | 59.5 | |
| Share FFS Medicaid | 5.8 | 9.8 | 1.6 | 2.9 | 5.1 | 1.0 | |
| Share Cash/Other | 1.8 | 2.7 | 1.2 | 4.0 | 4.7 | 2.8 | |
| Total prescriptions (N) |
110,045,188 |
132,843,714 |
|||||
Notes: IQVIA 2019 LRx Database extract for medication prescribed to treat either Asthma or Diabetes. Fill data collapsed to the prescriber zip code and then aggregated to tracts using population weights and HUD zip code to tract crosswalks.
Across tracts, prescription volumes in 2019 average roughly 1,300 for asthma and 1,600 for diabetes. These figures reflect the prevalence of both conditions and the regularity of medication use required for ongoing management. At the same time, wide standard deviations suggest wide variation, with prescribing activity more concentrated in more populated tracts. Mean days supplied per fill vary by condition: 36 days for asthma and 50 days for diabetes, consistent with differences in treatment regimens and refill frequency. Average mail order shares are 4.2% for asthma and 6.4% for diabetes, showing moderate variation across tracts but limited overall substitution away from retail pharmacies. At the national level, the tract-level aggregates correspond to approximately 1110 million total asthma prescriptions and 133 million total diabetes prescriptions in 2019.
Payer composition differs by condition. Medicare prescriptions account for roughly one-quarter of asthma fills and one-third of diabetes fills, reflecting the greater prevalence of diabetes in older adults. The majority of prescriptions are covered under third-party managed care arrangements, a category that includes commercial insurance and Medicaid managed-care organizations. Fee-for-service Medicaid represents a small share of total fills—about 6% for asthma and 3% for diabetes—while cash and other out of pocket transactions are uncommon, averaging below 5%.
Geographic patterns of mail order use
Figure 2 maps county-level mail-order prescriptions rates for asthma and diabetes in 2019, shown separately for all payers (panels 2A and 2C) and for Medicare prescriptions only (panels 2B and 2D). The all-payer maps suggests broad regional differences, with higher mail-order use across parts of the Upper Midwest, Mountain West, and New England, and lower rates throughout much of the South.
However, these spatial gradients reflect, in part, variation in insurance coverage. Focusing on Medicare (panels 2B and 2D) holds access to insurance fixed because Medicare provides near-universal coverage for adults aged 65 and older. When restricted to Medicare, the spatial pattern becomes clearer, with the Midwest and Mountain West exhibiting relatively high mail order rates. Focusing on the Medicare population, therefore, provides a consistent basis for comparing delivery-channel use across geographies while holding access to insurance fixed.
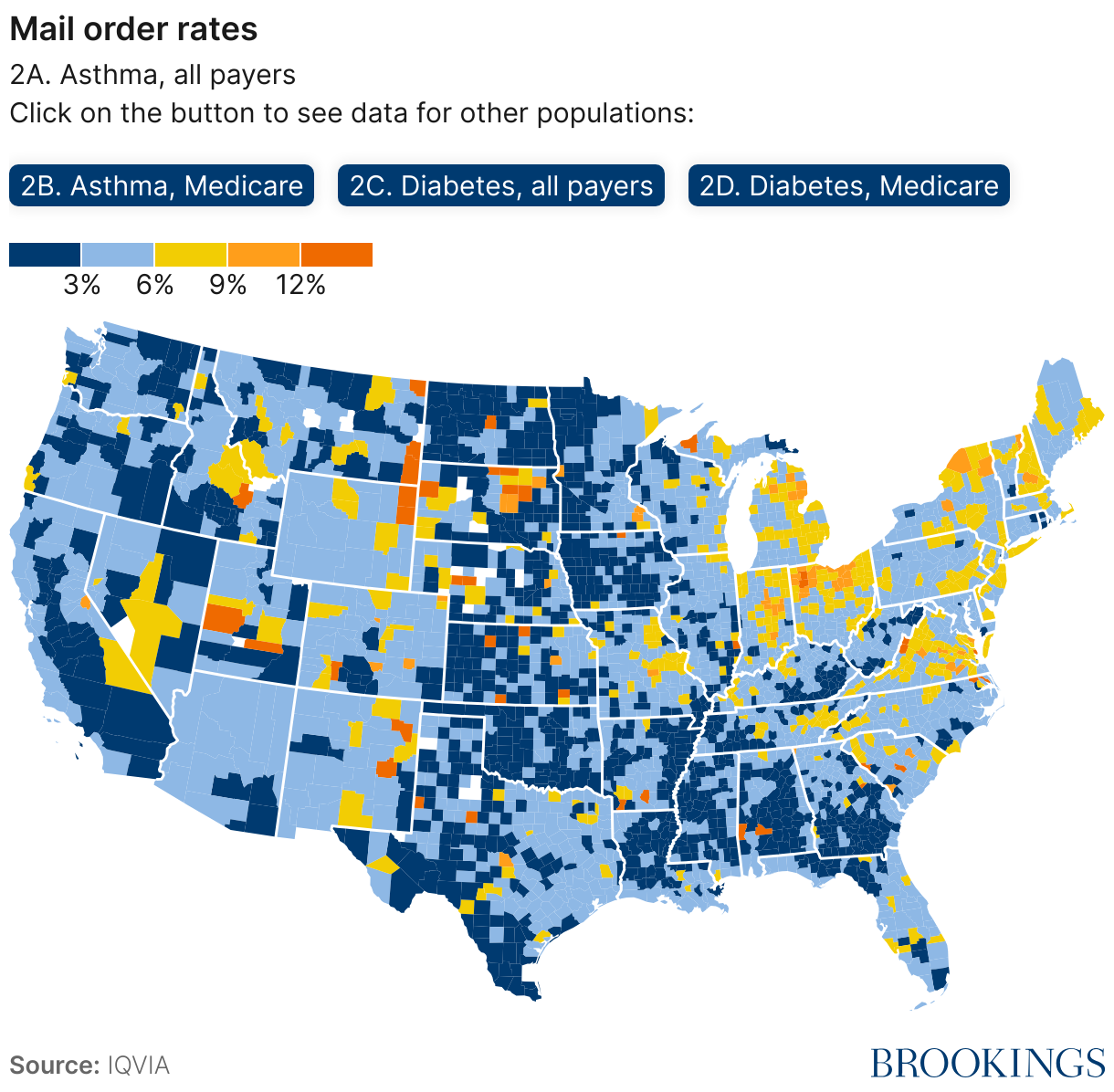
Table 2 reports Medicare mail-order shares for asthma and diabetes prescriptions by metropolitan status and proximity to the nearest pharmacy. This tabulation shows clear geographic regularities in which patients most strongly rely on mail delivery. Across all areas, mail-order use rises as distance to the nearest retail pharmacy increases. In large metropolitan tracts, mail-order rates average 5.2% for asthma patients and 7.5% for diabetes patients when a pharmacy is nearby, climbing to 6.7% and 10.0% when pharmacies are further away. Comparable gradients appear in small metropolitan and rural areas, though absolute differences are somewhat smaller. Mail-order rates are also consistently higher for diabetes than for asthma across all geographies, likely reflecting longer treatment duration and refill intervals.
|
Asthma |
Diabetes |
Tracts |
||||
|---|---|---|---|---|---|---|
|
Mean |
Median |
Mean |
Median |
Distance |
Number |
|
| Large Metro × Near pharmacy | 5.2 | 4.6 | 7.5 | 6.9 | 0.3 | 22,336 |
| Large Metro × Far pharmacy | 6.7 | 6.2 | 10.0 | 9.6 | 1.5 | 22,245 |
| Small Metro × Near pharmacy | 6.9 | 6.3 | 10.0 | 9.2 | 0.6 | 12,322 |
| Small Metro × Far pharmacy | 7.3 | 6.6 | 10.8 | 10.0 | 3.1 | 12,111 |
| Rural × Near pharmacy | 6.6 | 5.8 | 9.8 | 8.7 | 1.3 | 6,768 |
| Rural × Far pharmacy | 6.8 | 5.8 | 10.1 | 8.8 | 7.4 | 6,579 |
Notes: Mail-order rates are calculated from 2019 prescription transactions in the IQVIA LRx database. Distances to pharmacies are computed by the authors as straight-line distances between census-block centroids and retail pharmacy locations identified in 2019 in the National Plan and Provider Enumeration System (NPPES). Metropolitan categories (“Large Metro,” “Small Metro,” and “Rural”) follow the CDC National Center for Health Statistics (NCHS) urban–rural classification. Proximity (“Near” and “Far”) are defined as being below or above median distance to the nearest pharmacy, conditional on metropolitan category.
The relationship between pharmacy proximity and mail-order use is consistent across settings but differs in scale and meaning. In large metropolitan areas, the difference in pharmacy proximity between near and far tracts is small—about one mile (0.3 vs. 1.5 miles)—so higher mail-order rates in far tracts likely reflects convenience and time costs rather than limited access. In rural areas, by contrast, even near tracts are more than a mile from the closest pharmacy, and far tracts are more than seven miles from the nearest pharmacy. In these communities, mail delivery substitutes for local access rather than convenience, meaning that slower or less reliable postal service will be more likely to have direct consequences for medication access.
Pharmacy access and the geography of medication channels
The postal network forms an important component of the nation’s medication distribution system. Mail-order dispensing complements retail pharmacy access and offers a consistent channel for obtaining prescriptions where nearby options are limited. Understanding how local access constraints shape reliance on mail-order delivery helps clarify where the postal network plays the greatest role in ensuring consistent access to care.
Mail-order take-up and distance to pharmacy
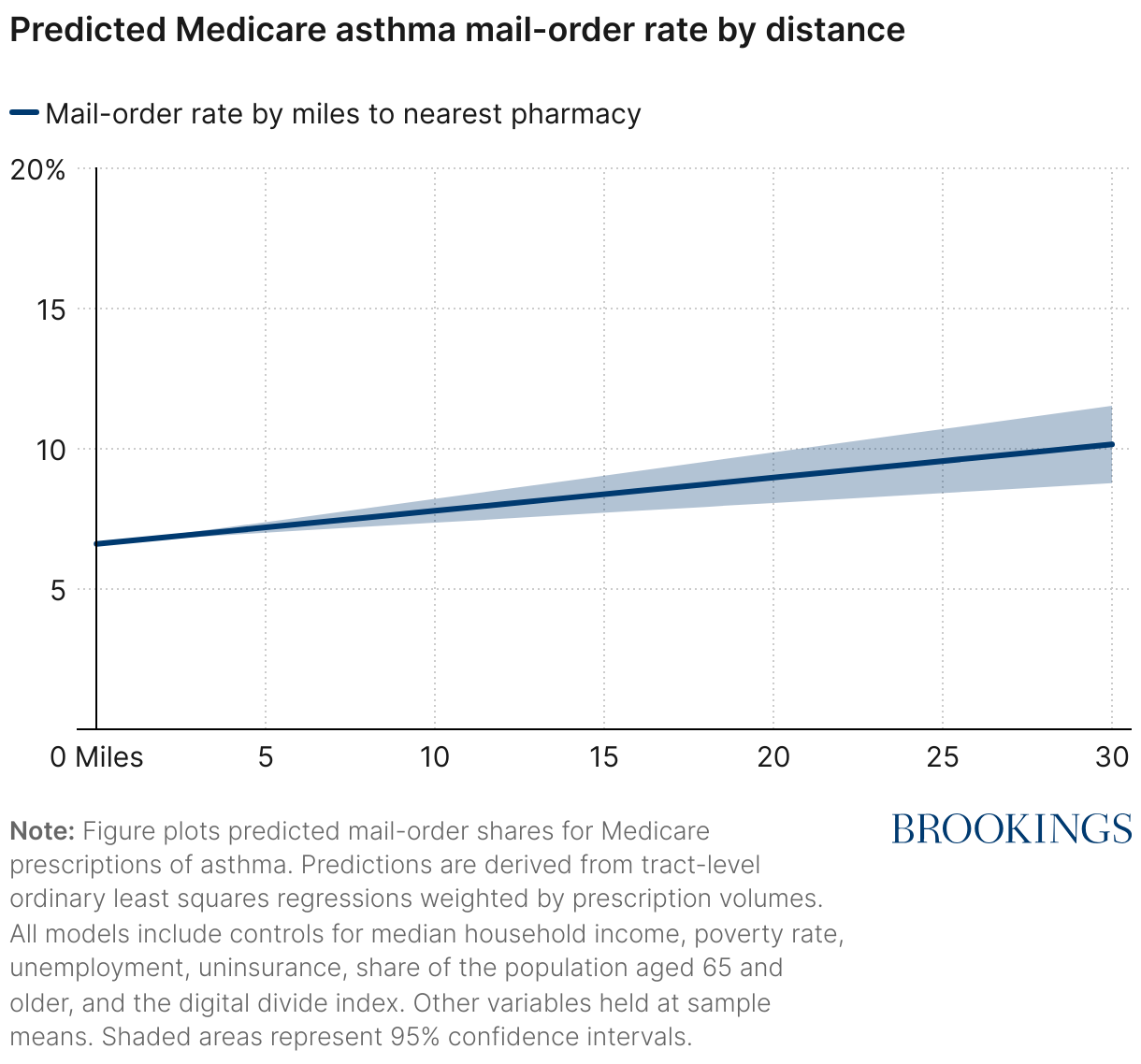
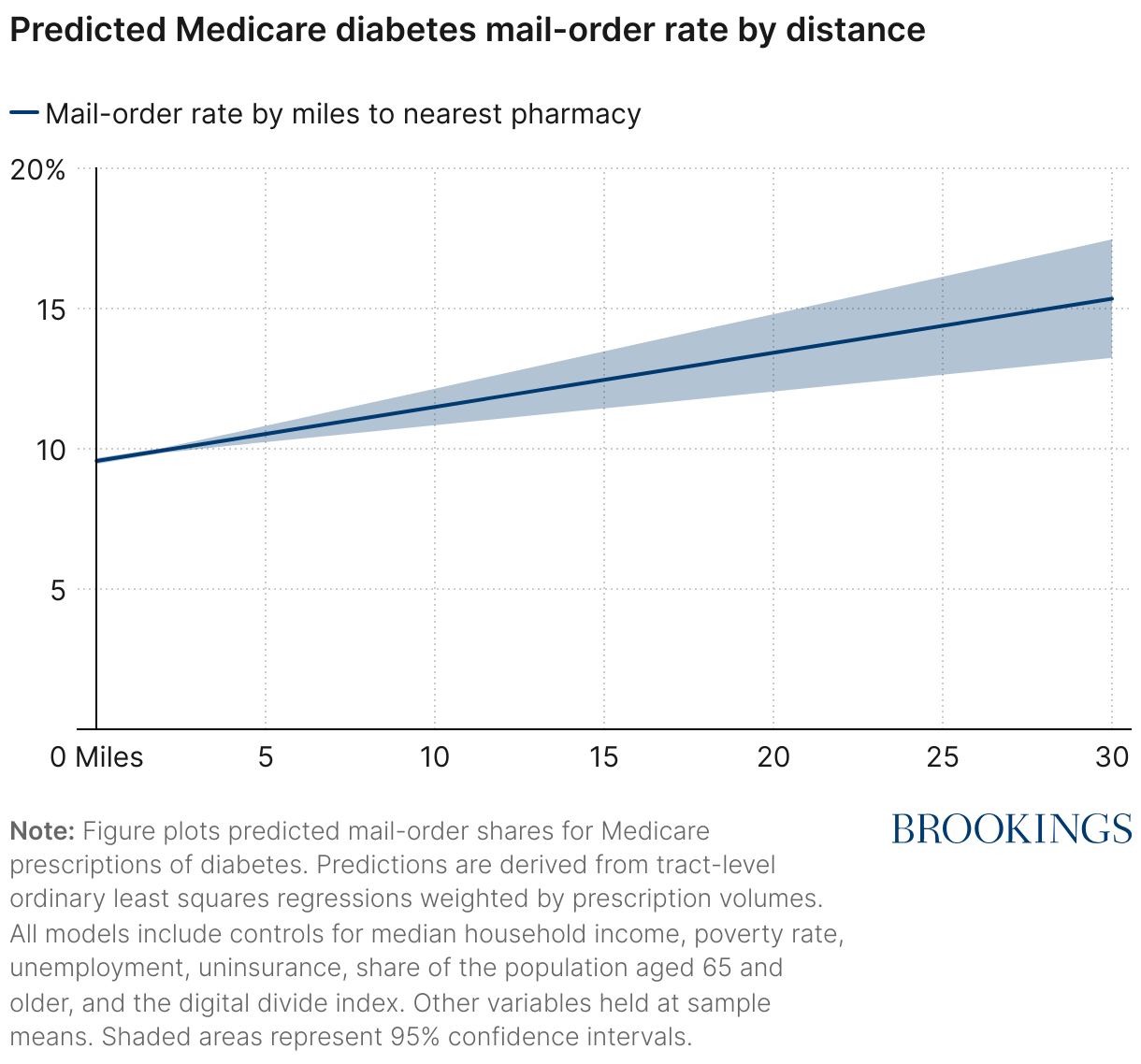
Figure 3 shows predicted mail-order shares for Medicare prescriptions of asthma and diabetes medication by distance to the nearest pharmacy, holding local socioeconomic and demographic characteristics constant.1 Mail-order utilization increases with distance: Each additional 10 miles from the nearest pharmacy is associated with a statistically significant increase in the share of asthma prescriptions of roughly 1 percentage-point and a 2 percentage-point increase in the share of diabetes prescriptions filled through mail delivery—equivalent to a roughly 20% increase relative to average take-up rates. These gradients remain statistically significant even after accounting for tract-level variation in income, poverty, employment, insurance coverage, digital connectivity, and age. Moreover, control variables follow expected patterns, with higher unemployment, higher uninsurance, higher poverty, and limited digital connectivity corresponding to lower mail-order use, and older tracts relying more heavily on delivery services (Appendix Table 1). These findings suggest that greater distance to pharmacies is consistently associated with increased reliance on postal delivery channels for prescription fulfillment.
FIGURE 3
Mail-order take-up rises with distance to pharmacy among Medicare prescriptions
Context: Pharmacy deserts and recent closures
Limited pharmacy access is not a fixed condition but one that evolves with market dynamics, including consolidation and store closures. Research documents that Black and Hispanic or Latino neighborhoods have consistently had fewer pharmacies per capital than predominantly white or diverse areas, reflecting structural inequities in the retail pharmacy landscape. Subsequent evidence from shows that these gaps have deepened as pharmacy closures accelerated between 2018 and 2021. Finally, estimates suggest that approximately 3% of the U.S. population, or roughly 10 million individuals, lives in a pharmacy desert, defined as a census tract that is far from a pharmacy and also high in poverty. While these tracts represent extreme access constraints, continued consolidation and closures will expand the number of communities facing limited retail access.
The postal system mitigates these pressures by providing a delivery channel that is insulated from local market dynamics. Through the Postal Service’s universal service obligation, mail-order customers retain access to prescription delivery regardless of geography or income. In this way, the postal network functions as a backstop for populations most affected by retail pharmacy closures. Where limited pharmacy access, high dependence on mail delivery, and postal network restructuring coincide, the resulting overlap creates concentrated risks for consistent medication access and continuity of care.
Identifying communities at the greatest pharmaceutical risk from the RTO
Finally, we introduce a new measure of prescription delivery vulnerability that identifies where multiple risks to medication access converge. Tracts are classified as “triple burdened” when three conditions occur together: (1) limited pharmacy access, based on distance to the nearest pharmacy and local pharmacy density relative to similar urban or rural areas; (2) heavy mail-order use, measured by the share of Medicare prescriptions filled through mail delivery; and (3) exposure to postal restructuring under the RTO plan, based on whether the nearest post office is affected by the RTO. These communities depend most on the postal network for prescription delivery and are also the places where slower or less predictable service is most likely to disrupt access.
Figure 4 summarizes the national distribution of tracts by the number of overlapping risks to prescription delivery. Nearly half of all residents live in areas facing at least one risk, while 6-7%—representing 3.7 million Medicare beneficiaries—reside in tracts classified as triple burdened. These figures illustrate that dependence on the postal network for prescription delivery is widespread and that a meaningful share of the population lives in places where that dependence coincides with potential Postal Service changes.
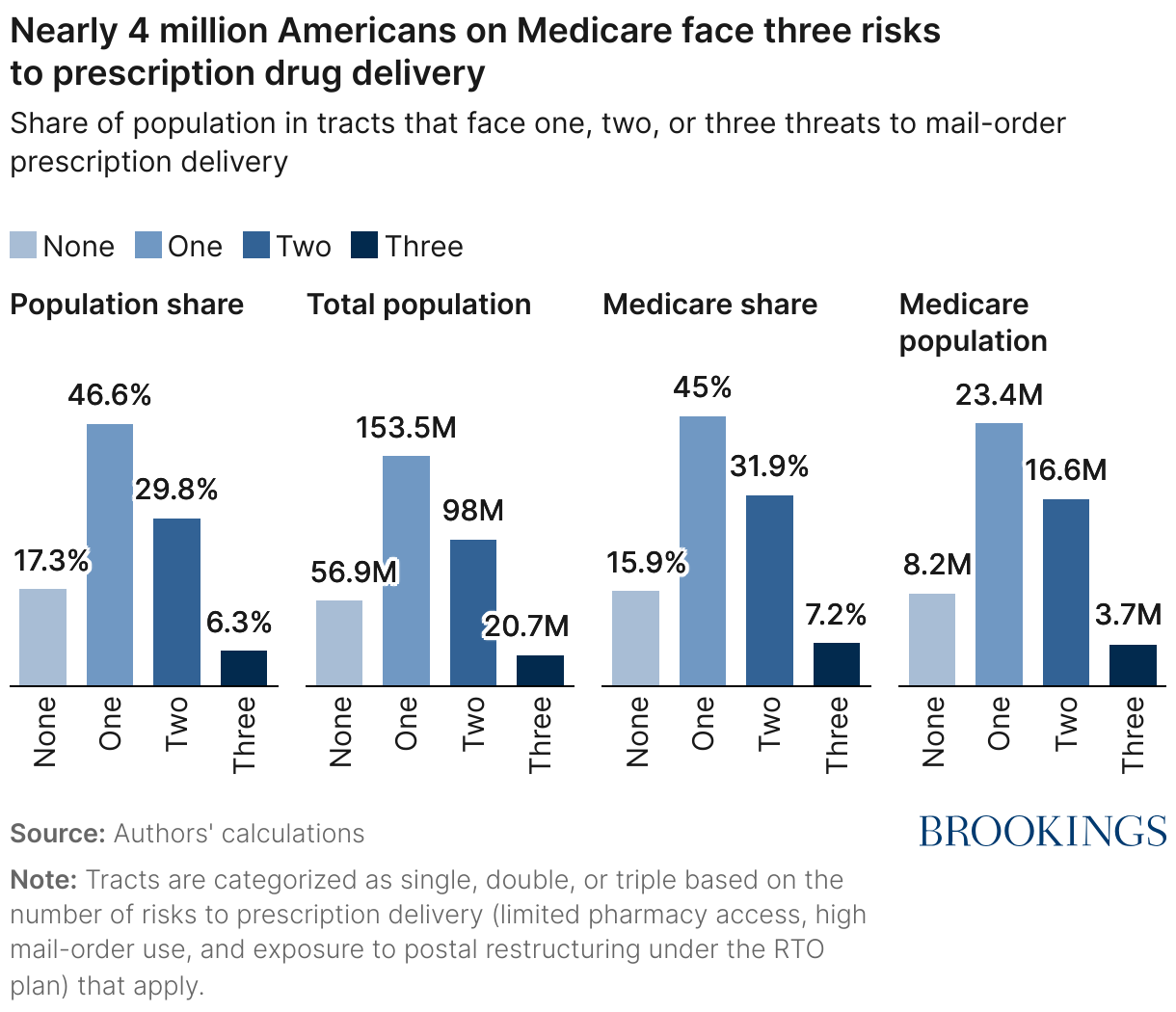
Table 3 describes community characteristics by the number of overlapping risks. Tracts with more risks tend to have older populations, longer distances to pharmacies, and higher rates of mail-order use, as well as near-universal exposure to RTO-affected post offices. These communities are somewhat more rural but not uniformly disadvantaged: Median income and education levels remain comparable to those of less-affected areas, suggesting that prescription vulnerability reflects geographic dependence on postal infrastructure rather than economic hardship in isolation.
|
Pharmacy Vulnerability Measures |
||||
|---|---|---|---|---|
| None | Single | Double | Triple | |
| Median household income ($) | 86,901 | 80,844 | 85,261 | 95,571 |
| Unemployment Rate | 6.0 | 5.8 | 4.9 | 4.3 |
| Below poverty line (%) | 14.3 | 14.7 | 12.0 | 9.4 |
| Bachelor's degree or higher (%) | 36.2 | 33.3 | 32.6 | 33.1 |
| Age 65+ (%) | 16.1 | 16.8 | 18.6 | 19.3 |
| Uninsurence Rate | 8.6 | 9.3 | 8.1 | 6.9 |
| Digital Divide Index | 17.7 | 18.7 | 18.8 | 18.2 |
| Rural (%) | 7.8 | 17.8 | 20.2 | 14.9 |
| Medicare Mail-Order, Asthma (%) | 4.5 | 5.5 | 8.4 | 10.7 |
| Medicare Mail-Order, Diabetes (%) | 6.6 | 8.1 | 12.4 | 15.7 |
| Distance to Pharmacy (Miles) | 0.7 | 1.2 | 2.9 | 4.2 |
| Population Affected by RTO (%) | 5.3 | 78.6 | 89.7 | 95.3 |
Notes: Tracts are categorized by number of overlapping risks to prescription delivery (limited pharmacy access, high mail-order use, and exposure to postal restructuring under the RTO plan. Tract characteristics are drawn from the 2023 ACS 5-year data. Digital Divide Index developed by Gallardo (2025)
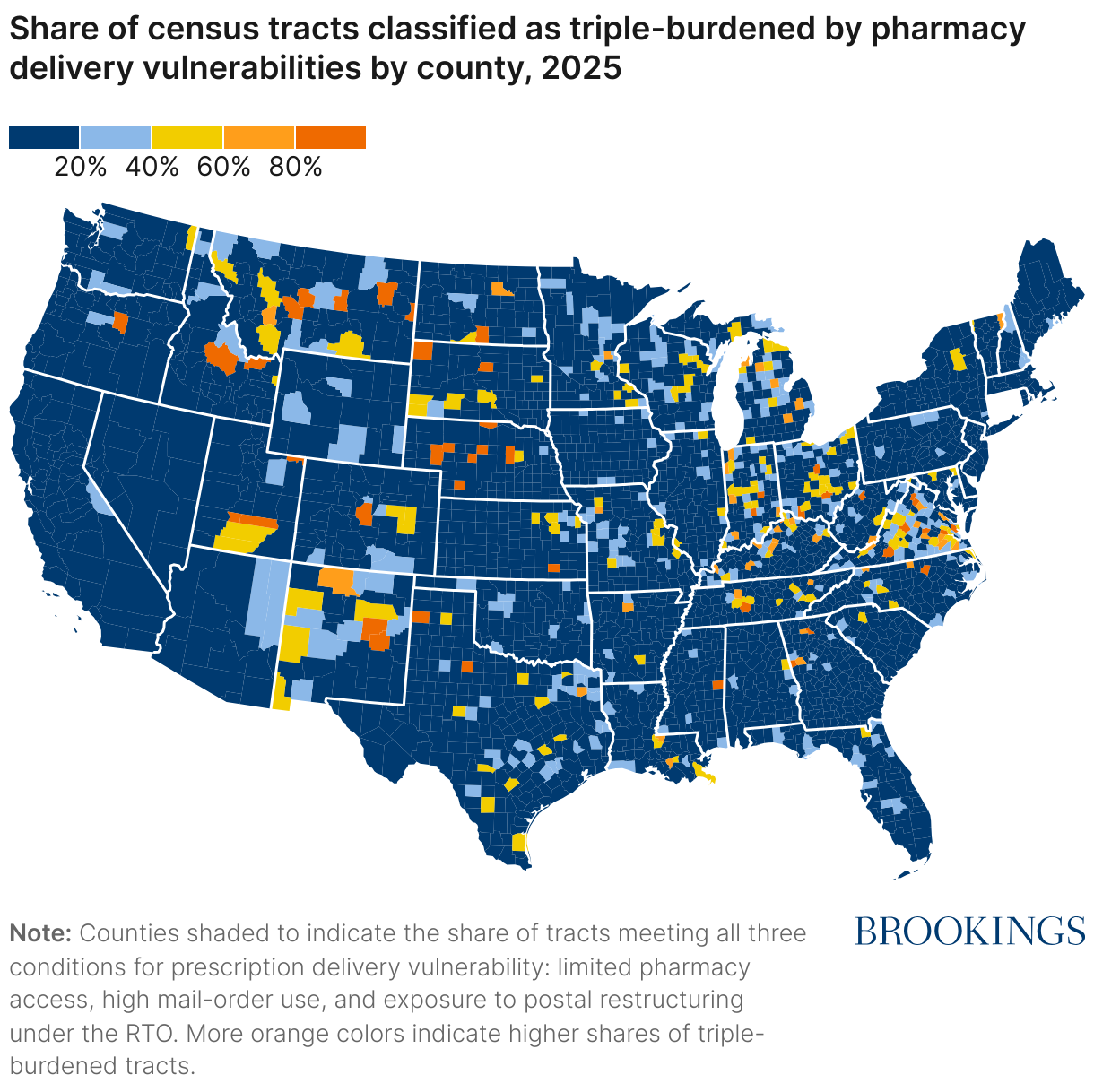
Finally, Figure 5 shows the geographic distribution of triple-burdened areas, illustrating where limited pharmacy access, high mail-order use, and exposure to postal restructuring coincide. The pattern is geographically uneven. Concentrations appear across the rural South, Appalachia, the upper Midwest, and portions of the Mountain West—regions where longer travel distances and widespread RTO implementation make communities more reliant on mail delivery for prescriptions. Other clusters that occur around small metropolitan areas may coincide with large populations of retirees with high mail-order and limited nearby pharmacy options. The map highlights how the operational footprint of postal changes overlaps with existing gaps in medication access, creating distinct pockets of prescription delivery vulnerability across the country.
Together, these results show that prescription vulnerability is both widespread and uneven. Most Americans face at least one form of risk to timely medication delivery, but a small subset of communities—about 6% of the population or roughly 3.7 million Medicare enrollees—depend almost entirely on the postal network for access to prescriptions. Because these areas are served by post offices undergoing operational change, even modest delivery slowdowns can have disproportionate effects on medication continuity, with implications for postal policy and the universal service obligation.
Conclusion
The postal network is not simply a logistics backbone—it is an essential component of the nation’s medication-delivery system. Mail-order pharmacies fill gaps left by retail closures, and they serve as a delivery channel with demonstrated long-run health benefits. Through longer refill intervals, automatic delivery, and reduced travel barriers, mail-order prescriptions improve adherence for treatment to chronic conditions and reduce avoidable hospitalizations and health care costs. These gains, however, depend on a single, often overlooked assumption: that mail arrives reliably, affordably, and on time.
The DFA plan is intended to strengthen the Postal Service’s operational consistency and financial footing through network consolidation and transportation optimization. Yet an independent analysis conducted by the PRC questioned whether the anticipated operational and financial improvements will materialize, while noting that resulting service slowdowns are likely to be unevenly distributed. The geography of the RTO rollout suggests that slower and less predictable delivery will be concentrated in areas most dependent on mail services for prescription access. For these communities, even small increases in delivery time can disrupt medication adherence and continuity of care. In this way, delivery speed is not merely a performance metric: It is a determinant of medication adherence and population health.
Viewed through this lens, the universal service obligation is more than an economic or operational standard. By ensuring universal, geographically neutral delivery, the universal service obligation performs a vital public health function. Its benefits—steady mediation access, greater adherence, and healthier outcomes—do not appear on postal balance sheets, yet they accrue across the health system.
The same logic extends beyond Medicare beneficiaries. Veterans, for instance, also rely heavily on mail-order prescription delivery. The Department of Veterans Affairs fills roughly four out of every five prescriptions through its Consolidated Mail Outpatient Pharmacy (CMOP) system, which “prepares, fills, and mails almost 84% of all VA prescriptions dispensed to Veterans throughout the United States.” Although some prescriptions are filled at local or retail pharmacies, this overwhelming dependence on mail-based delivery highlights that any erosion of postal performance reverberates through multiple federal health systems, not just Medicare.
Recognizing mail delivery as both a critical national infrastructure and a proven channel for sustaining long-term health underscores the stakes of postal reform. Maintaining the reliability and reach of the mail is not only a matter of efficiency or fairness. It is a condition for maintaining one of the nation’s quietest but most consequential health infrastructures.
Related Content



Authors


-
Footnotes
- Technical details about this analysis are provided in an appendix to this report.
The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).