Content from the Brookings Institution India Center is now archived. After seven years of an impactful partnership, as of September 11, 2020, Brookings India is now the Centre for Social and Economic Progress, an independent public policy institution based in India.
Coronavirus cases are quickly increasing across the globe, with just 580 reported cases (on January 22, 2020), in the span of a few weeks, the total number of confirmed COVID-19 cases have increased to over half a million across the world. The surge in coronavirus cases has crippled health systems in many countries, primarily due to shortage of hospital beds, manpower and equipment (personal protective equipment, ventilators etc). Countries affected by this severe problem responded in multiple ways – China built hospitals with thousands of temporary beds in a short period, the United Kingdom urged community members to volunteer with the National Health Service to tackle the problem.
The supply of essential resources (like manpower, protective gear) can be inelastic in the short term. However, this pandemic has revealed that one way to handle the increasing demand for healthcare is to ‘flatten the curve’. This is essentially achieved by social distancing which slows down the spread of disease and provides a much-needed breathing space to the health system (which has limited resources) to deal with rising number of patients. In other words, the purpose of these kind of interventions is to suppress and delay peak morbidity to ensure that the healthcare sector is not overwhelmed. However, for India, which aspects of the healthcare sector can be truly binding constraints in the short-run?
India confirmed its first case of COVID-19 on January 30, and in less than eight weeks the total number of cases has increased to 705 [1]. In our previous blog, we described how the limited number of hospital beds and ventilators is a serious concern for India. If the number of cases continue to rise at this pace, then temporary beds will be needed. There are already suggestions about converting hotel rooms and train coaches into make shift temporary hospital wards [2]. However, an absolutely binding constraint in the healthcare sector is that of doctors. A doctor takes approximately 6 to 12 years to acquire the necessary qualifications. Thus, the total stock of doctors in a country cannot be increased quickly in the short run. In this article, we look at India’s growing number of COVID-19 patients and compare it with the existing capacity of doctors, in order to forecast when India will face capacity limits in terms of available doctors to treat hospitalised COVID-19 patients.
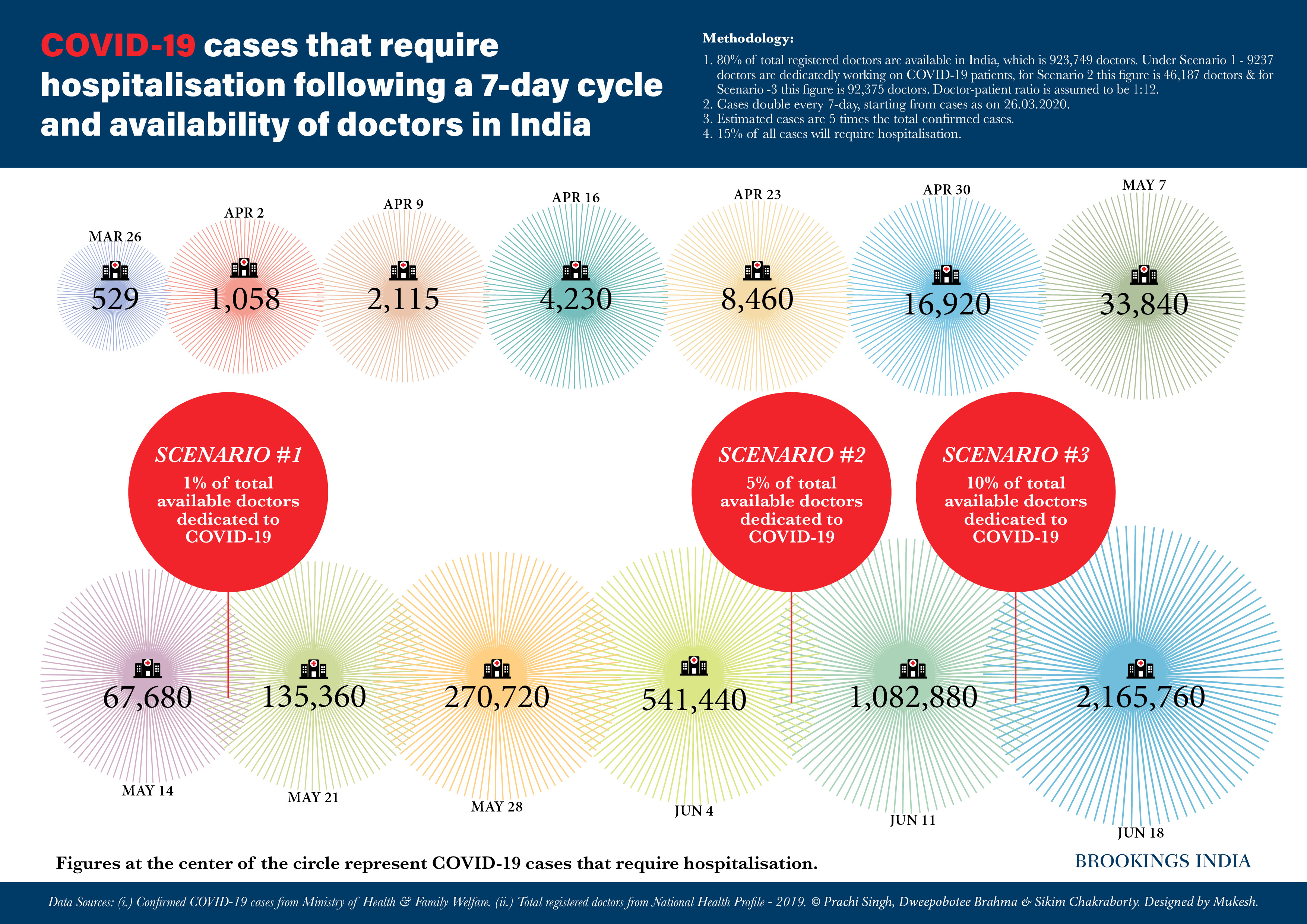
We use data on confirmed COVID-19 patients from the official statistics of the Ministry of Health and Family Welfare. The Government of India announced a nation-wide lockdown for three weeks, starting from March 25. The expectation is that this will slow down the disease transmission. In an optimistic scenario, this will lead to a doubling of cases at a slower pace, which we assume to be after every seven-days in our main analysis. We do a back-of-the-envelope calculation using a seven-day cycle where we extrapolate the number of confirmed cases for the next few weeks. Following existing epidemiology studies, we predict that the true cases are likely five-times the number of confirmed cases. Out of these, approximately 15% of cases will require hospitalisations [3]. We compare this number with the total capacity of the health system in terms of patients who can be treated by doctors available in India.
We use the number of total registered doctors from the National Health Profile 2019. Out of these, we assume that around 80% are available (on account of many doctors who might have migrated or retired), which includes doctors of all specialties including cardiologists, surgeons, general medicine etc. We consider three possible scenarios:
-
Scenario 1 where only 1% of the total number of available doctors are dedicated to treating COVID-19 patients,
-
Scenario 2 where 5% of the doctors are treating COVID-19 patients, and
-
Scenario 3 where 10% of the doctors are treating COVID-19 patients.
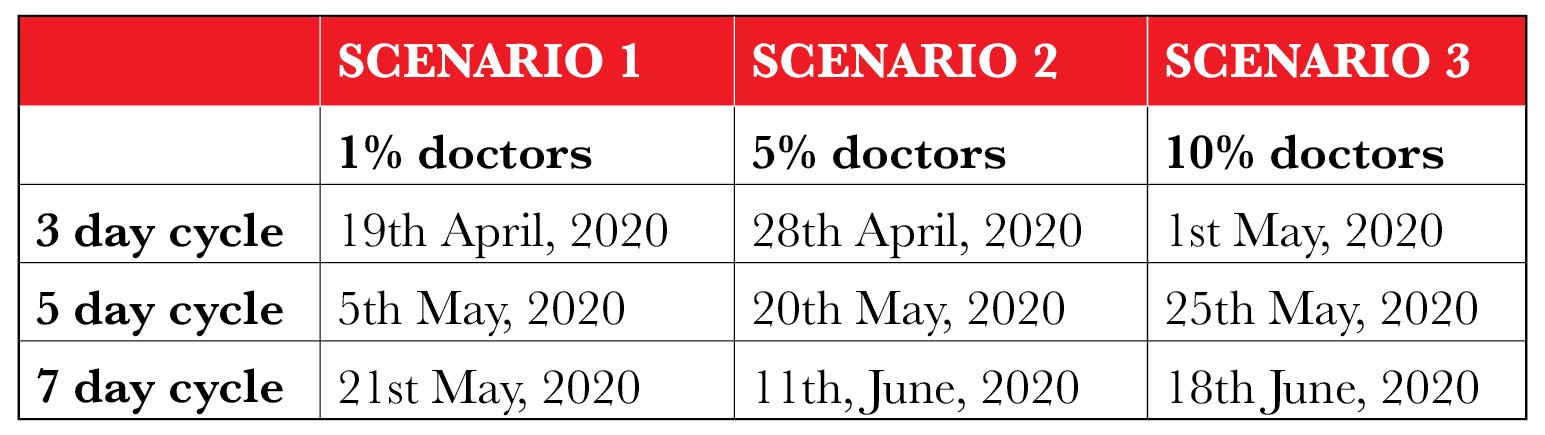
We assume that each doctor has the capacity to treat 12 hospitalised COVID-19 patients [4]. Thus, we arrive at a capacity constraint of treating 110,850 patients in Scenario 1; 554,249 patients in Scenario 2 and 1,108,499 patients in Scenario 3. Comparing our projections of hospitalised patients following the seven-day cycle with these capacity constraints, we conclude that India will reach the capacity constraint for doctors between May 14-21, 2020 under Scenario 1, between June 4-11, 2020 for Scenario 2, June 11-18, 2020, for Scenario 3.
We also provide results for alternate situations where we assume that the doubling of cases doesn’t slow down and follows a three-day cycle or a five-day cycle.
If we look at state-wise variation, different states will hit their capacity constraint in terms of doctors available to treat COVID-19 patients at different points of time. For example, Kerala with the highest number of COVID-19 patients as of now will be stretched in terms of doctor capacity by May 7, under Scenario-1. A similar analysis for Maharashtra, Karnataka & Uttar Pradesh reveals that doctors will be overburdened by May 21 (under Scenario-1) due to rising number of people who will require hospitalisation for treatment of COVID-19. In the short run, doctors from other specialities can also be mobilised to treat COVID-19 patients. To account for that, we have modelled two additional scenarios where 5% and 10% of doctors are treating COVID-19 patients. In fact, NITI Aayog has recently published a call for doctors to volunteer to treat COVID-19 patients [5].
Admittedly, the number of qualified trained doctors cannot be increased in the short-run. A complementary policy would be to train paramedical workers to conduct less skill-intensive tasks like routine check-ups, blood pressure monitoring etc., to take some of the load off the trained doctors. Unfortunately, COVID-19 pandemic does not stop patients suffering from other ailments from needing hospitalisation or even outpatient healthcare services. During this time, more patients, especially non-urgent ones, should be encouraged to use telemedicine services as much as possible. In this regard, NITI Aayog has recently published guidelines for practitioners to provide healthcare using telemedicine [6].
Notes:
[1] Ministry of Health and Family Welfare, cases as of 26.03.2020 at 3PM. https://www.mohfw.gov.in/
[2] BusinessToday article: https://www.businesstoday.in/sectors/auto/coronavirus-mahindra-maruti-ventilator-production-plan-reminds-of-world-war-ii/story/399302.html
[3] We have taken 15% as the projected hospitalisation rate for India. This number is 20% for China, where the older population was affected disproportionately higher. (Wu, Z., & McGoogan, J. M. (2020) “Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention.” JAMA).
[4] Karnataka’s Corona Task Force highlighted the need for 800 doctors to treat 9600 ICU patients (1 doctor per 12 patients). Anecdotal evidence also suggests that 10-15 patients are looked after by a single doctor. https://www.newindianexpress.com/states/karnataka/2020/mar/25/state-needs-to-gird-up-for-80k–cases-needs-4800-ventilators-2121251.html
[5] https://niti.gov.in/call-doctors-work-volunteers-covid-19-outbreak
Related Content



The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).

{kind=link}
Commentary
COVID-19 | Does India have enough doctors? An analysis of growing COVID-19 patients and existing medical capacity
March 27, 2020