
The COVID-19 pandemic was an exponential shock to much of the U.S. population and also exposed deep vulnerabilities associated with our fragmented health care system and our extreme income inequality. African Americans, for example, who suffer from racial as well as income inequalities, also suffered disproportionately from COVID-19 incidence and mortality. Predominantly black counties have COVID-19 infection rates that are nearly three times higher than that of predominantly white counties. According to the CDC, while they make up just 12.5 percent of the U.S. population, they account for 23 percent of COVID-19 deaths and are 3.5 times more likely to die from the disease compared to white populations.
This occurred for many reasons, including African Americans’ overrepresentation in “essential” jobs in the health sector and in transportation sectors where social distancing is impossible, their underrepresentation in access to good health care, and their higher probability of being poor. Longer-term systemic barriers in housing, opportunity, and other realms have exacerbated these problems. African Americans are also more likely to have preexisting health conditions such as asthma, diabetes, and cardiovascular diseases, which are all risk factors for COVID-19.
Presumably, then, African Americans should demonstrate the highest losses in terms of mental health and other dimensions of well-being. Remarkably, though, our findings suggest the opposite. We find that low-income African Americans remain the most optimistic of the race-income cohorts in our data and report significantly better mental health than their poor white counterparts. More generally, Hispanics and African Americans remain more optimistic than do whites in the face of the pandemic.
A recent nationally representative survey fielded by the Social Policy Institute at Washington University in St. Louis interviewed approximately 5,500 respondents from all 50 U.S. states from April 27 to May 12. It was internet-based and fielded through Qualtrics. Minorities were slightly overrepresented (13 percent of respondents were African American, while they make up 12.5 percent of the U.S. population, and 20 percent were Hispanic, while they make up 18 percent of the population; the survey also collected information on other racial groups). Respondents fell into four income groups, ranging from low to high income across all adult age categories and evenly split across genders.1 The survey had 200 questions covering demographics, employment, gig employment, assets, debt, financial status, well-being, food security, housing and other hardships, health, COVID-19 symptoms and perspectives about the pandemic, social benefits during COVID-19, and education.
Our analysis here covers two related areas of inquiry. The first is differential levels of life satisfaction, optimism, and reported mental health across race and income cohorts in the context of COVID-19. The second is how employment changes related to COVID-19 affected respondents’ well-being and mental health. Our econometric analysis was based on standard OLS regressions which controlled for socioeconomic and demographic variables such as age, gender, income, and education, as well as for unobservable differences across the states where respondents live.2
Related Content



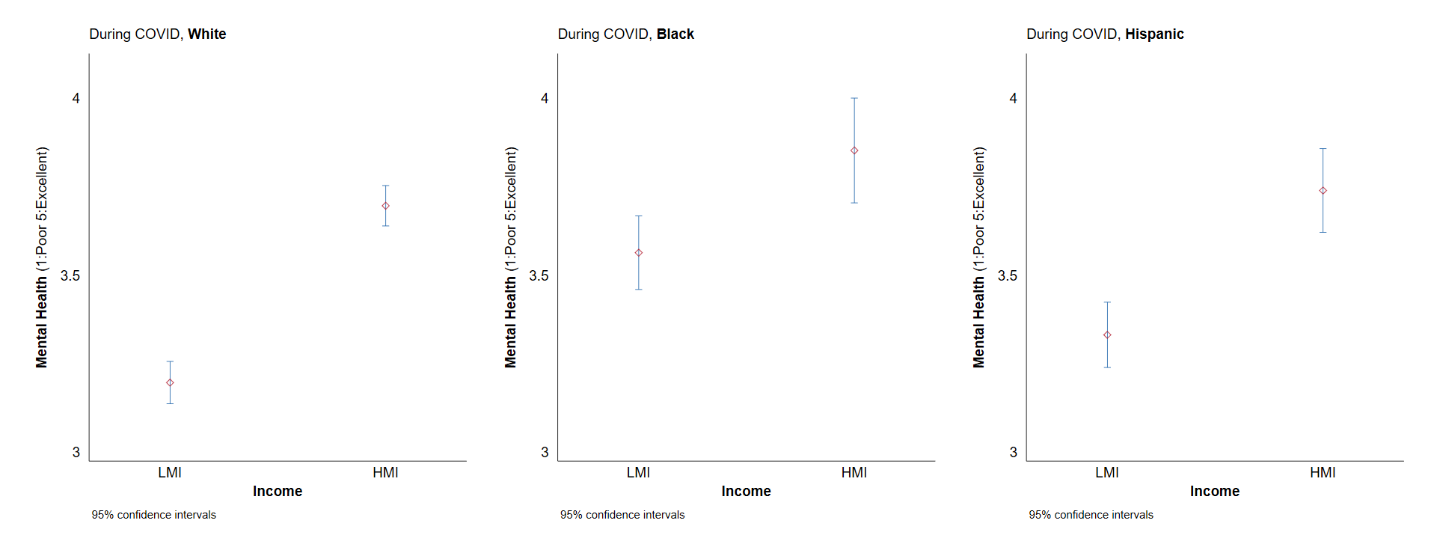
The first of our well-being variables is a standard life satisfaction question (based on the Cantril ladder) which asks: “Please imagine a ladder, with steps numbered from 0 at the bottom to 10 at the top. The top of the ladder represents the best possible life for you and the bottom of the ladder represents the worst possible life for you. On which step of the ladder would you say you personally feel you stand at this time?” Two following questions ask the respondent where they think they will be in three months and in five years, respectively. The latter two questions are designed to capture optimism and hope for the future. The second well-being variable documents the reported mental health of the same respondents. A first question asks respondents where their mental health ranked three months ago. The question has a five-point response scale ranging from poor to excellent. A second question then asks them to rank their mental health today on the same scale. We control for each respondent’s prior mental health and use their mental health today as the key dependent variable.
Our findings on race and income differences are, as noted above, remarkable. In keeping with the standard patterns in well-being, higher levels of income are associated with higher levels of life satisfaction and optimism. They are not, however, associated with significant differences in reported mental health. In contrast, there are large racial differences in well-being across races. The differences in reported life satisfaction—and particularly optimism for the future—between African Americans and whites are almost as large as those across income groups. African Americans also report better mental health than whites, with the most significant differences between low-income Blacks and whites. Hispanics also score higher on life satisfaction and optimism and have slightly better mental health than whites, but the gaps are not as large as those between African Americans and whites.3
Figure 1. General well-being measures (Cantril ladder), by race/ethnic group
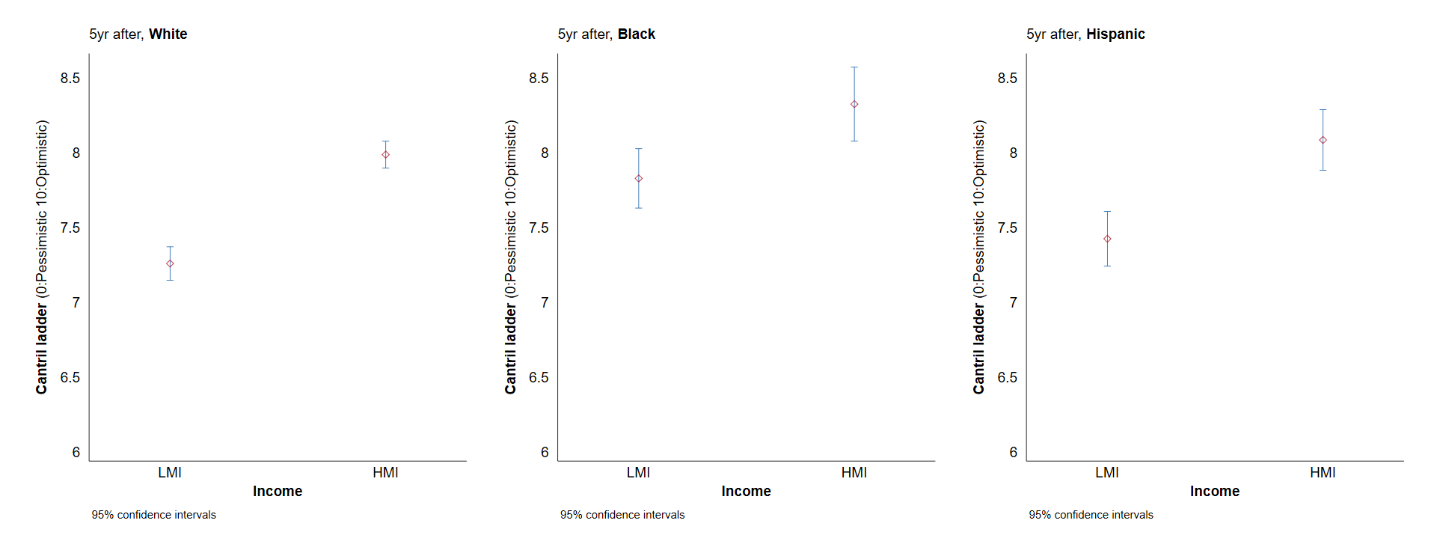
Figure 2. Mental health estimates, by race/ethnic group
These findings seem puzzling in the face of the objective disparities between low-income African Americans and other groups, as well as the disproportionate burden they have suffered from COVID-19. Yet they are remarkably consistent with patterns that we have previously found in the well-being of different race and income cohorts in the face of deaths of despair. Using over 1 million responses over five years from Gallup data for the U.S., we find large gaps in optimism and reported stress across poor African Americans and whites, with the former almost three times as likely to be a point higher on the 11 point optimism scale and 50 percent less likely to report experiencing stress the previous day than poor whites (poor Hispanics again fall in between the two groups on the same markers). This finding has stood the test of time, meanwhile, and did not change during and after the time of Trump’s election, for example.
While African Americans are more optimistic than whites in general in both sets of data, the largest differences are between poor Blacks and poor whites. Matching these metrics with CDC data on deaths of despair (suicide, drug overdose, and alcohol poisoning), we find they closely track the patterns in these deaths at the level of individuals, races, and places. African Americans and Hispanics are, for the most part, much less likely to be represented in these deaths than are whites.
Deaths of despair are, at least at some level, preventable as they are due to desperation-related behaviors. In stark contrast, COVID-19 is an exogenous shock—largely unrelated to individual behavior—that has hit African Americans disproportionately. Yet African Americans (and to some extent Hispanics) display the same high levels of hope and resilience in both instances.
The reasons for this resilience are complex. They include a historical trajectory of overcoming adversity, strong community ties, and continued belief in the promise of education at a time that it has faded among low-income whites. As a result, African Americans and Hispanics are gradually narrowing gaps in education and in life expectancy with whites. Poor whites, meanwhile, have fallen behind in absolute terms compared to wealthy whites and in relative terms compared to minorities, losses that are reflected in their high levels of despair. Historically, meanwhile, optimism among African Americans began to increase in the 1970s, when civil rights improved, and began to fall among less than college educated white men around the same time (coinciding with the first declines in manufacturing). It seems that the same traits that drive minority resilience in general are also protective of well-being and mental health in the context of the pandemic.
Related Books
Another surprising finding is that those respondents who report to have experienced COVID-19 symptoms, regardless of race or income level, are modestly more satisfied with their lives and more optimistic about the future than those who have not had symptoms. It may be that those who have experienced and gotten beyond COVID-19 symptoms have less fear about what is to come than those who have not (and they may also think they are not immune), and uncertainty is a key marker of ill-being. While we have data on those who tested positive for the virus, that sample (55 individuals) is too small to conduct meaningful statistical analysis.
Indeed, a key feature of COVID-19 is the uncertainty and deprivation it has brought to the lives of millions through the loss of employment. When we look at employment status—and changes therein—during COVID-19, we find that virtually all changes in status are worse for well-being and mental health than are keeping one’s employment. Yet we also find differences across those changes. Those respondents that experience a more lasting change—such as being permanently laid off or receiving a pay cut, experience more severe well-being effects than those who are temporarily laid off or have their work hours reduced (both of which signal a potential return to normalcy). As Table 1 shows, African Americans are more likely to have not had a job change and less likely to have been laid off, have hours reduced, or receive a pay cut. This may be because of their overrepresentation in essential jobs as in the health sector, grocery stores, and transportation (which are employment protective but increase the risk of disease incidence as it is so difficult to social distance).
Table 1. Job changes during COVID-19, by race/ethnicity
| White | Black | Hispanic | ||
| Not changed | 75.5% | 84.5% | 73.9% | |
| Changed | Temporarily laid off | 10.4% | 8.4% | 10.1% |
| Permanently laid off | 2.6% | 1.3% | 3.5% | |
| Work hours reduced | 5.6% | 3.4% | 7.0.% | |
| Pay cut | 2.0% | 1.0% | 2.7% | |
| Others | 3.9% | 1.5% | 2.9% | |
| N | 2,911 | 683 | 1,003 |
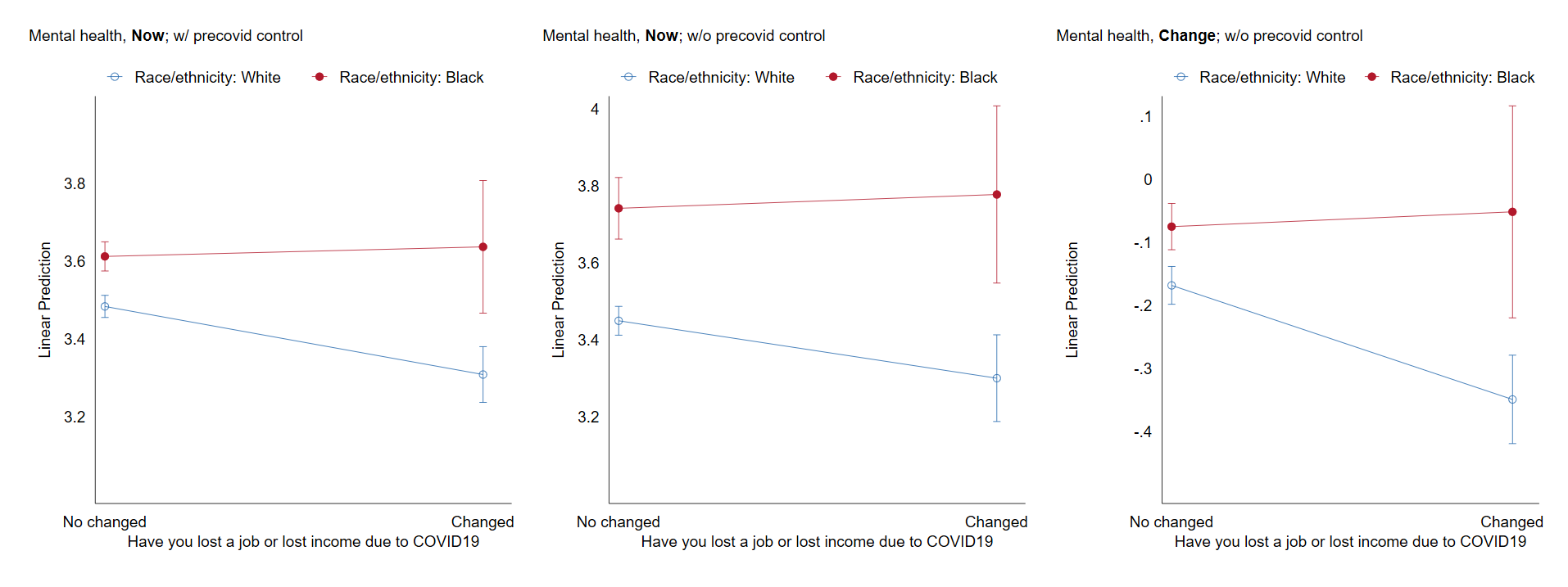
Yet again, though, African Americans stand out for their resilience to such shocks. When we simplify the breakdown to those who have suffered a change in job status and those who have not, we find that African Americans (across all incomes) who lost their jobs are both more optimistic and report better mental health than whites who have lost their jobs. This may be due to more experience with and adaptation to job insecurity among African Americans, or it may simply reflect general levels of higher resilience. Both traits are likely at play and seem to be protective of mental health in the same way they are in the face of other challenges, such as deaths of despair.
Figure 3. Marginal effects of job loss on general well-being measures (Cantril ladder), by race group (White vs. African American)
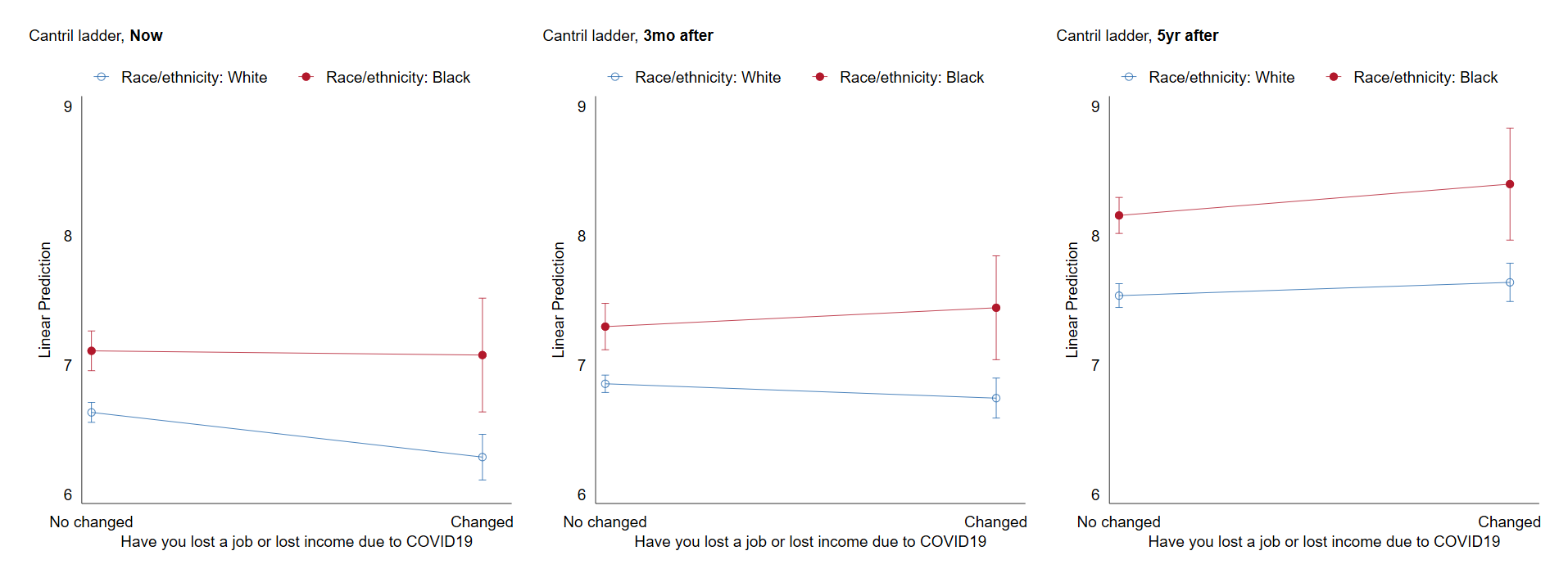
Figure 4. Marginal effects of job loss on mental health estimates, by race group (white vs. African American)
The U.S. ranks poorly compared to other countries in terms of protecting workers from COVID-19. Job loss is typically associated with a loss of health insurance in the U.S. and thus unemployment often produces a double shock introducing extreme uncertainty about the future (in addition there are also many people in jobs that do not provide health insurance and other benefits). In contrast in Europe and even in much of Latin America, most countries have national health systems that can be accessed regardless of employment status. And even with their more generous social welfare systems, many European governments have provided public support to companies that keep their workers on the payrolls, to avoid such large disruptions to both productivity and well-being.
Our findings on the well-being effects of COVID-19 highlight the highly unequal nature of our society—in incomes, health care, employment status, and race. The burden of COVID-19 on minorities, and particularly African Americans, is much higher than that on whites. It is also much higher for those with low-skill and/or insecure jobs with few if any benefits. The well-being costs for those in low-quality jobs are much higher than those with the capacity to remain in salaried jobs, and the benefit gaps across employment categories are far greater in the U.S. than in most other wealthy countries.
Perhaps the most important of our findings, though, is the high levels of hope and resilience of African Americans and Hispanics (although less so) compared to whites, despite being disproportionately impacted by the pandemic, both in terms of disease incidence and likelihood of being in essential jobs. Despite that, African Americans retain higher levels of resilience—more optimism and better mental health—than whites in the face of both. While this is not a well-known story, it is one with potential lessons for those coping with COVID-19-related uncertainty and other challenges. And at a time that U.S. society is facing unprecedented challenges due to the dual “pandemics” of COVID-19 and racial injustice, it is time to better understand the roots of African American resilience, as those, in turn, will play a vital role in healing our deeply divided society going forward.
In addition to her affiliation with Brookings, Michal Grinstein-Weiss is a professor and the head of the Social Policy Institute at Washington University in St. Louis.
Authors




-
Footnotes
- We constructed our income group based on self-reported annual household income in 2019, household size, and areal median income (AMI) at the county level. Low income: household income < 80 percent AMI. Moderate income: 80 percent AMI ≤ household income < 120 percent AMI. Middle income: 120 percent AMI ≤ household income < 170 percent AMI. High income: 170 percent AMI or more.
- We clustered our standard errors at the state level. As a robustness check, we also ran the same equations with state dummies and the results were essentially the same, with the exception of reduced significance on some of the employment status coefficients. We chose the former specification to avoid over-restricting the 5,000-person sample with 50 state dummies.
- The CDC’s “pulse” survey, conducted from late April to early June, found that Blacks reported increased anxiety during this period). While they reported less anxiety than Hispanics and “other” racial groups, they reported more anxiety than whites. The question in the CDC survey is quite different from either the optimism or mental health in general ones that we use. It is: “Over the last 7 days, how often have you been bothered by the following problems … Feeling nervous, anxious, or on edge?” Clearly it is plausible that anxiety might increase at the intersection of COVID-19 and widespread protests against racial discrimination, but that optimism could remain high at the same time. In addition, the pulse data combines all income groups, while the differences that we find, as is clear from the figures below, are greatest between low-income Blacks and whites.

