
The COVID-19 virus was the third leading cause of death in 2020 after heart disease and cancer, claiming approximately 375,000 American lives. As a result of this pandemic, U.S. life expectancy declined by a full year-and-one-half, according to The National Center for Health Statistics. But for specific racial groups the drop in life expectancy has been more pronounced. Black and Latino or Hispanic people experienced a staggering 2.9- and 3-year downturn in life expectancy, respectively, compared to 1.2 years for white people.
Substantial changes in life expectancy have long been a bellwether for trends in the overall health of our nation. And as a general macro trend, life expectancy in the United States (and worldwide) has trended upward over the last several decades, according to a 2020 U.S. Census report. That same Census report also optimistically estimates that U.S. life expectancy will reach an all-time high of 85.6 by 2060.
Understanding life expectancy declines caused by COVID-19 provides an opportunity to spotlight racial and health disparities related to the pandemic and beyond. The pandemic exacerbated existing disparities in work, education, housing and health care. In this paper, we use a social determinants of health framework to explore some of the factors contributing to why Black and Latino or Hispanic individuals have experienced a noticeably larger decline in life expectancy over the last year.
COVID-19 disparities in infections, deaths
The CDC reports COVID contraction rates by race, comparing American Indian, Alaska Native, Black and Latino or Hispanic persons to white people. Black, American Indian or Alaska Native, and Latino or Hispanic individuals are more likely to contract the virus than white Americans, and they’re also more likely to be hospitalized and die should they contract the virus. These disparities help explain why, when accounting for age, Black, Native American or Alaska Native, and Latino or Hispanic people together make up 60.5% of COVID-19 deaths despite only making up 32.8% of the age-standardized population. Despite historic attempts by a biased scientific community to provide an empirical grounding for racial hierarchies—scientific racism—there is no compelling evidence that genetic or biological differences between racial groups drive racial disparities in health outcomes.

The lingering effects of scientific and de jure racism call for another window into understanding measurable racial health disparities. Analyses must address the social conditions that influence health, a set of predictors that researchers refer to as the “social determinants of health” (frequently referred to by the acronym SDOH.)
Understanding what we mean by social determinants of health
The U.S. Department of Health and Human Services (HHS) defines the social determinants of health as “the conditions in the environments where people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.” The department lists five main categories for these social determinants: economic stability, education access and quality, health care access and quality, neighborhood and built environment, and social and community context.

As an example of this framework, HHS notes that “environmental pollutants can cause health problems like respiratory diseases, heart disease, and some types of cancer” and that “people with low incomes are more likely to live in polluted areas and have unsafe drinking water.” In the context of the pandemic, these social determinants are particularly important in evaluating pre-existing respiratory issues that increase vulnerability to the effects of the virus.
Social determinants interact to influence mortality and morbidity, but they flow directly from sociopolitical structures, a concept clearly communicated by the World Health Organization’s Commission on Social Determinants of Health in their 2008 report on global health equity. The report notes that “unequal distribution of power, income, goods, and services” leads to “unfairness in the immediate, visible circumstances of people’s lives—their access to health care, schools, and education, their conditions of work and leisure, their homes, communities, towns, or cities—and their chances of leading a flourishing life.” The report also argues that the “unequal distribution of health-damaging experiences is not in any sense a ‘natural’ phenomenon but is the result of a toxic combination of poor social policies and programmes, unfair economic arrangements, and bad politics.”
Many researchers make a distinction between determinants that people interact with in neighborhoods —schools, environmental pollutants, housing, etc.—and those that people do not necessarily face directly: tax policy, government processes, school financing. For this analysis we use an inclusive definition of social determinants, which include state, regional or national factors. Regardless, social determinants are not natural, inevitable, or necessary and consequently neither are the health disparities they produce. We could collectively choose to change the policies, practices, and conditions that degrade people’s quality of life. The failure to do so is a morally weighted choice.
Social determinants and COVID-19
By exploring correlations between social determinants and COVID-19 health outcomes, we can get a clearer picture of the factors that have led to such disparate outcomes. In keeping with the framework outlined by the World Health Organization and HHS, we identified five key determinants: 1): labor force participation and employment; 2): health care access and insurance; 3): housing security and density; 4): environmental exposure; and 5): food access and nutrition.
The key determinants we discuss in this paper should not be thought of as independent or mutually exclusive. The determinants are structurally interconnected in important ways. For example, employment status has direct implications for health insurance access, since half of all Americans get their health insurance from their employer. Nevertheless, the key determinants provide a useful framework for thinking about the broad range of socioeconomic factors that affect health outcomes.
Labor risks
We examine labor force participation and employment type as leading social determinants for two reasons. We know that Black, Native American or Alaska native, and Latino or Hispanic workers are overrepresented in the low-status, essential workforce and are more likely to work in high-risk, in-person workplaces. In addition, these essential workers are underpaid and often without benefits like health insurance. This overrepresentation is associated with higher excess mortality.
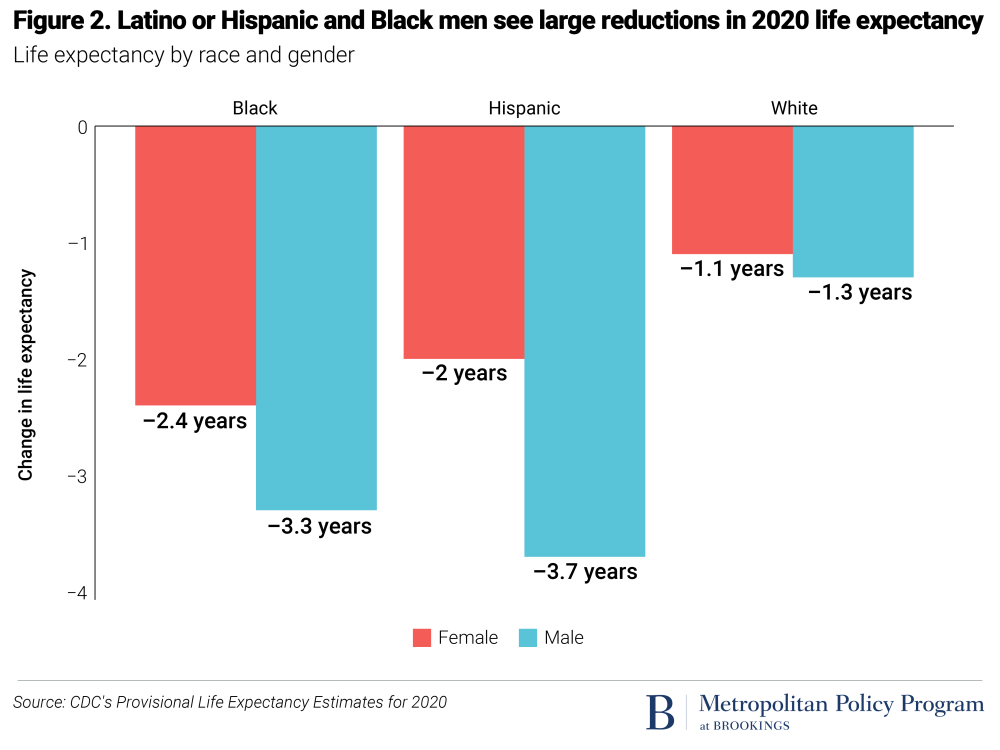
Another reason we expected to see employment patterns as a critical indicator is because of the sharp gender disparities by race in pandemic-fueled life expectancy declines, as depicted below. We theorized that these gender disparities could be explained, in part, by connecting them to labor force participation. Latino or Hispanic men experienced the steepest decline in life expectancy with a 3.7-year drop followed by Black men at 3.3 years, Black women at 2.4 years and Latino or Hispanic women at 2 years.
In support of this hypothesis, our research finds that Latino or Hispanic men and Black women have the highest labor force participation rates for men and women, respectively. And while all groups’ labor force participation rate dropped during the pandemic, from February 2020 to February 2021, Black and Latino or Hispanic men’s labor force participation rate dropped the least.

There is much more that needs to be explored about gender disparities in life expectancy, an issue recently raised by our colleagues. But given these findings, Latino or Hispanic and Black people—especially men—continued participation in essential and frontline jobs during the pandemic is the likely reason life expectancy decline was so pronounced for these groups.
Health insurance
In examining health insurance status as a determinant, we started with the observation shared in a 2020 Brookings report that “health and health care have a two-way relationship. Poor health care leads to poor health, which then makes health care more expensive and less accessible.”
Families without regular access to a trusted primary care practitioner are less likely to seek medical care when COVID-19 first strikes. And when families needed to access primary care physicians for the first time during the pandemic, they had a median wait of up to 10 days. Kaiser Family Foundation notes that for the uninsured “is not designed to provide the same comprehensive access and protection from high medical bills COVID-19 treatment as traditional insurance.” Thus, if families do need to seek out medical care for COVID-19 symptoms, they may be responsible for paying tens of thousands of dollars if they are under- or uninsured. This causes fear which fosters mistrust in the health care system that delays the relationship building that is necessary for successful care.
A study published by the Clinical Infectious Diseases journal last November finds strong correlations at the county-level between insurance rates and COVID-19 cases and deaths. Lack of health insurance is thus likely a driver of poor health leading into the pandemic, which rendered people more vulnerable to the negative effects of the virus. In addition, a lack of insurance likely amplified negative outcomes during the pandemic, for example by discouraging people from receiving treatment until their condition required hospitalization.
Our research depicted below finds that the percentage of Black, Latino or Hispanic, and Native American people with health insurance is less than the percentage of white people, as well as the overall U.S. percentage.

We also find that Black, Latino or Hispanic, and Native American workers are less likely to receive employer-sponsored health care compared to other workers, as shown below.

In addition, a 2020 Brookings analysis finds lower uninsured rates for Black and Latino or Hispanic essential workers, and researchers at the Urban Institute also found in 2020 that insurance rates are substantially lower for American Indian or Alaska Native and Latino or Hispanic frontline workers. Moreover, since health insurance is so often tied to employment, it compounds the disadvantage for people who have lost jobs during the pandemic.
Despite the dampening effects of increased vaccination on both the number and severity of COVID cases, insurance status continues to be an important social determinant for COVID-19 health outcomes. According to a report by the Kaiser Family Foundation, almost a quarter of unvaccinated adults in the United States are uninsured. And recent ABC News research shows states that are currently dealing with a surge in cases tend to have higher uninsured rates.
Housing insecurity and density
Black neighborhoods experience greater housing insecurity than neighborhoods with different racial and ethnic compositions. Black majority neighborhoods see elevated eviction rates and foreclosures, regardless of other factors across the nation. A study from the Joint Center for Housing Studies found that Black and Latino or Hispanic renters are much more likely to be cost-burdened and fear eviction.
A 2018 review of the literature from Health Affairs finds that aside from the negative health outcomes of being unhoused, “People who are not chronically homeless but face housing instability (in the form of moving frequently, falling behind on rent, or couch surfing) are more likely to experience poor health in comparison to their stably housed peers.” PLoS One found that foreclosures and housing instability leads to “[increased] degradation of the neighborhood environment [which has] indirect, cross-level adverse effects on health and mental health.” The concentrated evictions and foreclosures in Black neighborhoods and the housing instability present in Black and Latino or Hispanic neighborhoods leads to negative health outcomes for families and entire communities.
Providing low-income families access to affordable housing isn’t just necessary, it also helps combat negative health outcomes during and after the COVID-19 pandemic. A study from the Center for Outcomes Research and Education found that after families were moved to affordable housing, Medicaid expenditures decreased by 12%. At a time when hospitals across the nation are at, or near capacity, and becoming unhoused is exceedingly linked to negative health outcomes during the pandemic, creating affordable housing for families is of utmost importance.
Lastly, we considered the presence of multiple generations in the same home. While during normal times, multi-generational housing allows extended families to spend valuable time together, during the COVID-19 pandemic this type of housing exposes older adults to higher risks. These housing situations have concentrated risks in specific communities. We have previously showed how Black majority neighborhoods have much higher rates of multi-generational family cohabitation.
Related Books
At the household level, Latino or Hispanic households have much higher rates of adult children living at home, while Black and American Indian or Alaska Native households have higher rates of families who live in a household with a nonadjacent, or “skipped,” generation—a grandparent. All minority groups have higher rates of three generational housing than do white households.

Environmental exposure
As part of its working definition of environmental justice, the U.S. Environmental Protection Agency (EPA) emphasizes fair treatment: “No group of people should bear a disproportionate share of the negative environmental consequences resulting from industrial, governmental and commercial operations or policies.” Unfortunately, this vision of fair treatment is more of an aspiration than a current reality. Too many parts of the nation have not responded to the many decades of discriminatory policy and systemic racism that have led to contemporary inequities regarding the built environment. For example, a recent study of 108 U.S. urban areas published in the journal Climate finds that places formerly discriminated against in redlining and other housing policy are disproportionately exposed to heat waves through lack of greenspace and the high presence of impervious surfaces such as concrete.
One core dimension of environmental justice is access to clean air—a necessity for good health outcomes particularly in the context of the pandemic. And as with many kinds of growing inequalities, respiratory health varies based on socio-economic status. A recent study published by the American Medical Association finds that “income- and education-based disparities in respiratory health have persisted, and potentially worsened, despite secular improvements in air quality and tobacco use, suggesting that the benefits of these improvements have not been equitably enjoyed.” In particular, the study, published in JAMA Internal Medicine, found persistent and widening “socioeconomic disparities in respiratory symptoms, lung disease prevalence, and pulmonary function”; disparities which were attenuated but not eliminated when controlling for smoking rates. The study was based on a repeated cross-sectional analysis of national health examination surveys conducted from 1959 to 2018 that included 160,495 participants. This fits with a meta-review of the literature on socio-economic status and air quality correlations which finds similar patterns across the United States as well as globally.
While class is certainly an important variable in understanding access to clean air, race is perhaps an even more important variable. Our analysis depicted below finds that there is a greater correlation between the presence of respiratory hazards and the size of Black/Hispanic population than the correlation between those hazards and income and poverty. We estimated correlation coefficients for the several community metrics and the EPA National Air Toxics Assessment Hazard Quotient. We looked at data from the 192 largest metropolitan areas, which covers 78% of the nation’s population. These data show the Respiratory Hazard Quotient has a higher correlation with the percentage of Black and Latino or Hispanic residents than neighborhood poverty and a greater absolute correlation than median income.

However, because Black and Latino or Hispanic people are concentrated in certain metropolitan areas, we followed Howell and Korver-Glenn’s methodology of using the ratio of the percentage of Black and Latino or Hispanic neighborhood residents to the percentage of Black and Latino or Hispanic metropolitan residents. This significantly reduced the effects of these neighborhood characteristics without eliminating them. Using this methodology eliminated the difference between the Black-Latino or Hispanic and poverty correlations, meaning that, even accounting for metropolitan area differences, Black and Latino or Hispanic neighborhood population is as correlated with toxic air quality as poverty.

This analysis is further supported by a study published in Science Advances on racial disparities in exposure to fine particular pollutants which found that “most emission source types—representing ~75% of exposure to PM2.5 in the United States—disproportionately affect racial-ethnic minorities. This phenomenon is systemic, holding for nearly all major sectors, as well as across states and urban and rural areas, income levels, and exposure levels.” In addition, a preprint study from medRxiv finds strong correlations between fine particulate matters and COVID-19 death rates.
While we focus here on air quality given the connections to COVID-19 as a respiratory virus, but it is just one form of toxicity exposure. A publication by the Innovation Frontier Project examines the larger array of environmental toxins including hazardous waste and finds that “African American, Hispanic, and low-income families disproportionately live and attend school near pollution sites.” These exposures undermine public health, particularly during pandemics, but also during normal times when Black, Latino or Hispanic and American Indian or Alaska Native households see higher comorbidities leading to lower labor force participation and higher death rates.
Food access, nutrition, and health
When it comes to food, access, consumption, and quality are all closely related to life expectancy. For example, a recent study published in Nutrition found that both increases in healthy food expenditure and decreases in unhealthy food expenditure were associated with increases in life expectancy.
Access to healthy food is also closely tied to diseases like hypertension, obesity, and diabetes, all of which disproportionately affect Black and Latino or Hispanic individuals in the U.S. These diseases have been identified as leading comorbidities of COVID-19, meaning those who have them tend to have worsened COVID-19 outcomes. Discussion of these comorbidities invites us to think about the connections between nutrition and health—but those connections need to be further contextualized within social determinants like food access and food security.
To understand food as a social determinant, we first need a clear picture of contemporary trends in food insecurity which are different than in previous eras. As a 2020 report by the White House Conference on Food, Nutrition, and Health notes, “while calorie malnutrition in the U.S. has been largely eradicated, changes to our food system accompanied by increasing economic inequality have created a crisis of diet-related obesity, diabetes, and other chronic diseases, and widened other disparities in the accessibility and affordability of nutritious foods.”
Similarly, in a recent report, our Metropolitan Policy Program colleagues show that even before the pandemic, “After years of steadily declining food insecurity rates—10.5% of U.S. households still faced food insecurity.” As expected, “This rate was highest among households with incomes below the poverty line (34.9%).” The authors also note that “Latino or Hispanic and Black households experienced food insecurity rates of 15.6% and 19.1%, respectively—disproportionately higher than white households (7.9%).”
There is often a geographic component to food insecurity, but the commonly held belief that food insecurity is caused by a lack of supply (“food deserts”) does not fit with our colleagues’ analysis. Instead of a supply issue, they argue that it is a demand issue, and specifically that low-income households do not have enough money to purchase the level of food (and at the optimal nutritional value) required to fully meet their household needs. In other words, food insecurity is affected by the legacy of racism in the labor market.
The federal government’s Supplemental Nutritional Assistance Program (SNAP), whose recipients are disproportionately Black and Latino or Hispanic, is meant to address this economic issue. In theory, SNAP is designed to help families near or below the federal poverty line afford a healthy diet. But in practice, SNAP is often insufficient for low-income families to sustain healthy diets because the benefits are based on an outdated model of food consumption and pricing.
As further evidence for understanding food security and access to nutritious food as primarily an economic issue, our colleagues find, Households that spent their first [child tax credit] CTC payment tended to spend it on food, and food insufficiency (comparable to very low food security) rates among respondents dropped 3% immediately after the first wave of CTC payments was dispersed.” This finding emphasizes the importance of finding correct root causes for comorbidities, rather than blaming people for poor decisions regarding diet that they were constrained to make due to lack of money. The success of the CTC payment in helping address this issue also provides a good starting point for thinking what it means to design policy interventions that are informed by SDOH frameworks.
Conclusion
Increases in life expectancy are not inevitable. And indeed, even before the pandemic, life expectancy trends in the U.S. have not been entirely positive. In March 2020, just as America was first beginning to grapple with the pandemic, Princeton economists Anne Case and Angus Deaton published their book, Deaths of Despair and the Future of Capitalism, which examines deaths from suicide, drug overdose, and alcohol abuse, whose collective impact has led to drops in life expectancy in recent years.
Case and Deaton’s research offered a conceptual framework that has shaped the way we understand the ongoing opioid crisis including here at Brookings. Yet much of the media coverage of their research and of the opioid crisis still centers on white people—and especially on white men. This is emblematic of our nation’s history: We present white men as a normative and universal reference point in our medical research while sidelining or outright ignoring other racial groups even when those groups are suffering from the same trends often compounded through layers of racial bias and inequity.
The ongoing COVID-19 pandemic has placed a spotlight on the racial disparities in health outcomes in America, as well as the underlying socioeconomic factors that give rise to them. Even though the largest declines in U.S. life expectancy caused by COVID-19 may be behind us, health disparities caused by the social determinants outlined in this paper will continue to manifest themselves unless they are addressed. The introduction of highly effective vaccines has offered a path to overcoming the pandemic, but many of the social determinants discussed in this paper are also leading to significant differences in vaccine access and uptake.
The acute economic distress caused by the pandemic and its recession has led the federal government to implement a series of unprecedented policies that have begun to address some of the underlying socioeconomic disparities discussed above. Over the last year and a half, the government has sent out three rounds of economic impact payments, significantly enhanced unemployment insurance benefits, expanded the child tax credit, implemented an evictions moratorium, and enhanced SNAP benefits. These programs offer a good start to addressing the racial disparities noted above. In fact, there’s evidence that many of them have disproportionately benefited Black and Latino or Hispanic families, since they are more likely to experience economic, food, and housing insecurity. New data from the U.S. Census Bureau show that the federal stimulus checks kept two million Black and Latino or Hispanic children out of poverty last year. The expanded Child Tax Credit is projected to slash child poverty across all racial groups, but Black and Latino or Hispanic children are among those who would see the largest declines in poverty rates.
Many of these programs have already expired or are set to expire soon. The eviction moratorium expired July 31, unemployment insurance benefits expired the first week of September (many Republican-led states cut the benefits even earlier), SNAP enhanced benefits expired on September 30, and families are no longer receiving economic impact payments. The abrupt end to many of these programs amid the evolving pandemic, which has regained force due to the Delta variant, has left many at risk of losing their homes or going hungry.
Permanent policy solutions are needed to address the underlying causes of racial disparities in health outcomes. As the next health crisis inevitably comes along, we cannot expect a different result unless we work to better understand and address the socioeconomic roots of racial disparities in health outcomes.
Related Content



Authors





