This analysis is part of The Leonard D. Schaeffer Initiative for Innovation in Health Policy, which is a partnership between the Center for Health Policy at Brookings and the USC Schaeffer Center for Health Policy & Economics. The Initiative aims to inform the national health care debate with rigorous, evidence-based analysis leading to practical recommendations using the collaborative strengths of USC and Brookings. This article originally appeared in Health Affairs on April 10, 2017.
Secretary of Health and Human Services (HHS) Dr. Tom Price and Centers for Medicare and Medicaid Services (CMS) Administrator Seema Verma face significant decisions across a range of programs in the first half of 2017. Decisions regarding how the new Administration will approach the health insurance marketplaces rightly command the most attention, but important decisions on payment reform loom as well.
In particular, the Administration must soon decide whether to continue with the large-scale demonstration projects testing bundled payments for hip and knee replacements, hip fractures, bypass surgery, and heart attack. Secretary Price and others have criticized these models on a number of grounds, most importantly that they require all providers in selected geographic areas to participate. The Administration recently delayed the start date for the newer cardiac bundles program, raising some questions as to whether HHS will proceed with the program under its current structure.
We argue there is some scope to modify these models to address concerns raised by Secretary Price and others without damaging the integrity of the models. In particular, there is room to address concerns about the role of hospitals relative to physicians in the models. However, making these models optional would eliminate the ability to generate robust evidence on their effectiveness, dealing a severe blow to efforts to use bundled payments to improve care delivery in orthopedics and cardiac care, and to the chances for bringing bundled payments to scale nationally in the coming years.
THE PROMISE OF BUNDLED PAYMENT
In recent years, bundled payments have gained increased prominence through several large-scale tests and pilots by the CMS Innovation Center and private payers. The allure of bundled payments is in explicitly unifying responsibility for both the financial and patient outcomes associated with a clinical episode under a single provider, giving that provider an incentive to coordinate care during the episode.
Related Content



One prototypical use of bundled payments is for knee replacements. Under fee-for-service, a hospital is paid for the cost of nursing, equipment, devices, and other items and services furnished during a surgery; physicians and other clinicians are paid separately for professional services delivered before, during, and after the surgery; and post-acute care providers are paid separately for nursing and rehabilitative care. No single provider is responsible for the entire experience, and so patients often experience fragmentation, including confusion at discharge, lack of follow-up care, inadequate rehabilitation, and avoidable medical complications, emergency room utilization, and readmissions.
In a bundled payment arrangement, however, one of those entities is held responsible for the entirety of a patient’s care during an episode, including ensuring that the patient receives high-quality and efficient care from the other participants in the delivery chain. Different bundled payment arrangements designate different “quarterbacks”—generally referred to as the “episode initiator”—among the major participants, but the hospital and the surgeon are the most common.[1]
MEDICARE’S EXPERIENCE WITH BUNDLED PAYMENT
Before 2010, the history of bundled payment arrangements was one of small-scale tests by Medicare and other payers. These tests, including the Medicare Participants Heart Bypass Center Demonstration during the 1990s and the Medicare Acute Care Episode test, generally found savings without harming quality of care, but they were limited in their scope. Given their potential, after passage of the Affordable Care Act, CMS invested significantly in four new types of bundled payment projects from 2013-2016, all of which are still ongoing (see Exhibit 1).
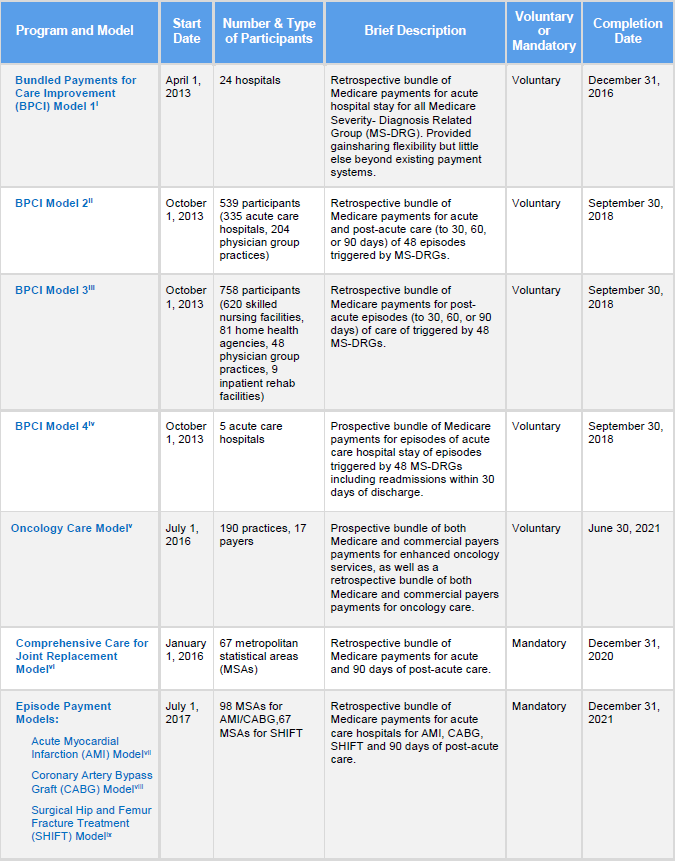
Two of these models are voluntary, meaning that they include only providers who elect to be paid under the alternative structure being tested:
Bundled Payments For Care Improvement Initiative (BCPI)
This project was launched in 2013 to test 48 inpatient episodes across a diverse set of providers. For the first time, it allowed physicians, nursing facilities, and other post-acute care providers to become “episode initiators.” Additionally, BPCI added an option for “conveners” to hold financial risk on behalf of providers who wanted to participate but could not carry the requisite risk or administrative overhead. As of April 2016, BPCI had more than 1500 participants, including 385 acute care hospitals, 283 physician group practices, and 681 skilled nursing facilities. The program is scheduled to end on September 30, 2018. The independent evaluation has not yet yielded a definitive answer as to whether BPCI will achieve its goals. Orthopedics bundles and, to a lesser extent, cardiac bundles have shown positive financial results, while others are more mixed.
Oncology Care Model (OCM)
This project pays oncology practices a monthly management fee for patients undergoing chemotherapy for a range of cancers. Practices provide an enhanced level of service with this fee and adhere to evidence-based treatment guidelines. Practices that meet quality objectives and achieve savings, including for drug expenditures, for a given year receive a performance-based payment in addition to the enhanced services fee. The program began in July of 2016 and will end in 2021. Currently, 190 practices accounting for approximately 150,000 Medicare patients are participating nationwide.
For reasons discussed in detail below, CMS also deployed two “mandatory” models that encompass all hospitals in specified geographic areas:
Comprehensive Care For Joint Care Model (CJR)
In 2015, CMS announced this model, which requires participation from hospitals in 67 randomly selected markets for hip and knee replacements and nearly all associated care for 90 days following discharge. Covered care includes both rehabilitative and physical therapy services provided in hospital, nursing facility, and home health settings. Target prices are initially based on a hospital’s historical costs but transition to a regional average over several years. The target price is set at an initial discount, generally three percent, so that Medicare reaps its savings before payment; providers can receive shared savings only if they beat the discounted target price. The discount can be reduced by improving performance on a composite measure of clinical quality. More than 800 hospitals are participating in the model, which began its first performance year in April 2016.
Cardiac Bundles, A.K.A. The Episode Payment Model (EPM)
Shortly after finalizing the CJR project in 2016, CMS proposed and finalized new mandatory bundled payments for bypass surgery and acute myocardial infarction in 98 randomly selected market areas across the country. The agency also extended the services included in the 67 CJR markets to include treatment for hip fractures. Like the CJR model, hospitals are held responsible for their financial performance against a target price and their performance on a handful of quality measures, including clinical processes of care and patient experience measures. Under a recent interim final rule HHS delayed the beginning of the first performance period from July 1, 2017 to October 1, 2017, and solicited comment on whether the delay should extend to January 1, 2018. More than 1000 hospitals are participating in this model.
Through rulemaking for the cardiac bundles program, CMS also added an option for clinicians in the CJR or cardiac bundle to qualify for the five percent bonus as an Advanced Alternative Payment Model under the Medicare Access and CHIP Reauthorization Act (MACRA).
THE PATH AHEAD FOR MANDATORY BUNDLED PAYMENT MODELS
The combination of CJR, BPCI, OCM, and EPM have greatly increased the scope of CMS’ overall bundled payments portfolio. With the significant increase in scale and the introduction of mandatory elements, bundled payments encountered their first significant political resistance, particularly from some hospitals and from some Republicans in Congress.
Hospitals generally opposed a mandatory model test, preferring a voluntary structure. Physician groups were somewhat more positive, though the major associations representing orthopedic surgeons expressed concern that the models’ approach to risk adjustment did not adequately account for differences between higher and lower risk patients.
Patient and consumer groups generally supported the stronger push from CMS on bundled payments. Members of Congress weighed in on both sides, with many Republican Members, including now-Secretary of HHS Tom Price, expressing concern about any mandatory model. Some argued that this type of demonstration project was an infringement of Congressional authority over Medicare. Still, some Members supported the project as advancing the cause of payment reform in Medicare.
Below, we consider two issues to which Secretary Price objected for the CJR and EPM projects: the question of whether they must be mandatory; and the appropriate role for physicians relative to hospitals in bundled payment models.
SHOULD CJR AND EPM CONTINUE AS MANDATORY MODELS?
Our view: It is important to try mandatory models for bundles as well as other payment initiatives.
Purely voluntary models like BPCI have important weaknesses that make them unlikely to generate the evidence required to take bundled payment arrangements to scale in Medicare or elsewhere. The first is limited size. Although BPCI was the largest test of bundled payment models yet conducted, many episodes had too little volume to generate statistically precise estimates of the model’s effects with respect to those conditions.
Another weakness of voluntary models is selective participation. The providers electing to participate in BPCI were atypical in a range of ways—for example, BPCI participants were in markets with twice as many specialists per capita as non-BPCI markets. This left the program vulnerable to criticism that any observed differences in performance in the program reflected underlying differences between participants and non-participants, rather than actual care redesign spurred by the model. By contrast, the random assignment methodology used by CJR and EPM completely avoids this problem. In principle, random assignment could be used in a purely voluntary model by allocating some of the providers who volunteer to participate to the control group. This approach, however, would exacerbate the sample size concerns noted above.
Selective participation also limits the generalizability of the results of a model test. Even where the other statistical challenges posed by selective participation can be overcome, a voluntary demonstration can typically only provide reliable evidence on how a model affects the types of providers who elect to participate. If bundled payments are ever to reach national scale in Medicare or elsewhere, we will need evidence that they work for all providers, not just “early adopters.” Policymakers will also benefit from evidence on how the effects of models differ when all providers in a market participate, rather than just a few, as these models’ systemic effects may differ from their effects on individual providers.
Mandatory approaches also facilitate the use of model designs that have potential to drive larger improvements in the efficiency of care. In particular, there is a strong rationale for setting common spending benchmarks for all providers in a geographic area based on the area’s average costs historically. Setting common benchmarks creates a level playing field across providers and allows market forces to drive market share to the most efficient providers, a potential source of major cost savings. Setting common benchmarks is also often viewed as more equitable.
In voluntary programs, however, setting common benchmarks for all providers can keep historically high-cost providers from participating (which narrows the scope of the model’s potential impact), while providing a windfall to historically low-cost providers (which creates a significant fiscal cost). To avoid this problem, voluntary programs typically must tailor benchmarks to the historical experience of each prospective participant by “rewarding” historically higher-cost providers with higher benchmarks and “penalizing” historically lower-cost providers with lower benchmarks.
The Administration’s options for making the CJR and EPM models “less mandatory” are relatively limited. The Department could mandate a small payment reduction (e.g., three percent for eligible services) for hospitals that do not participate. But this would compromise the design significantly and could still be viewed as punitive. The agency could dial back the number of selected markets, but the sample size of the existing models is near the minimum required for an effective evaluation. In addition, paring back the number of markets or the number of hospitals participating will also reduce the number of opportunities for specialist physicians to participate in Advanced Alternative Payment Models that qualify for a five percent bonus under MACRA.
Moreover, it would send a damaging signal to the health care industry about CMS’ ability to carry out mandatory demonstrations if the Administration backs away from bundled payments in CJR and EPM, sharply curtailing the potential effectiveness of the Innovation Center. In addition, such a retrenchment could have ripple effects for private payment reform efforts that attempt to complement CMS programs. Eschewing mandatory models would also have a fiscal cost. The Congressional Budget Office (CBO) told Congress in October of 2016 that prohibiting the Innovation Center from undertaking mandatory demonstrations “would substantially reduce the savings from [the Center’s] activities” because of the significant advantages such demonstrations have in certain cases.
SHOULD THE TREATMENT OF PHYSICIANS UNDER MANDATORY BUNDLED PAYMENT PROGRAMS BE MODIFIED?
Our view: CMS can expand physicians’ role in bundled payment models while maintaining their structure.
Another criticism of CJR and EPM is they are too “hospital-centric” — that is, by placing financial responsibility with hospitals, they give them too much power relative to other provider types. There are at least two reasons to question this premise, however. First, precisely because hospitals are at risk by default and clinicians are not, the negotiating table starts in a configuration favorable to clinicians. Hospitals need engagement from clinicians to succeed in the model, while clinicians could, in theory, maintain practice as usual, absent a favorable agreement with the hospital.
Second, the voluntary BPCI program, in which physician groups can participate as episode initiators, has precedence over the CJR and EPM programs. Accordingly, physician groups initiating joint replacements, hip fractures, or selected cardiac procedures and treatments can claim a bundle before a hospital can. About 280 physician groups participating nationwide in the BPCI program would be able to take advantage of this arrangement, with potentially more coming online if CMS follows through with its stated intent to re-open the next generation of BPCI in 2018.
Related Books
For these reasons, we believe the current program treats physicians equitably. However, if the Administration desires, HHS does have options to allow physicians to take more financial risk for bundles, enhancing their primacy under these models. Physicians could be allowed to, on a voluntary basis, step in front of the hospital and accept ownership of CJR or EPM bundles, as the American Medical Association, Society of Thoracic Surgeons, and Academy of Orthopedic Surgeons have proposed. This could be accomplished without undercutting the superior evaluation design of the CJR and EPM projects if hospitals remain responsible in the absence of a physician initiator. However, allowing physicians to claim more episodes would aggravate the existing hospital participants by depriving them of potential savings opportunities. A variant of this concept would be to allow “convener” organizations to step in between CMS and physician groups, holding risk for the latter to facilitate more widespread participation, as was allowed in BPCI.
Another option for allowing physicians to take some financial risk for CJR and EPM bundles is to maintain the mandatory nature of the programs, but spread responsibility to all participants in an episode of care in proportion to the portion of a care they provide — an approach sometimes called a “virtual bundle.” This would put physicians and post-acute care providers directly at risk. How this would change the efficacy of a bundled payment model is uncertain. The overall payment associated with an episode would not change; the only difference would be in how that payment is allocated among providers. As a result, it is possible that providers would negotiate similar agreements with one another under either structure, leading to similar outcomes. However, it is also possible that this approach would create confusion about who is accountable for the outcome of any given patient, undermining efforts to change practice patterns, particularly since it would arguably attenuate incentives for providers most able to affect outcomes.
CONCLUSION
The Department of Health and Human Services has several options for addressing Secretary Price’s prior objections to the hospital-at-risk structure of the CJR and EPM models that could maintain the integrity of these payment reform initiatives. In our view, however, the Department does not have a good alternative to the mandatory structure used for CJR and EPM that could preserve the integrity of the models tests and the scope of their potential impact. Making these models optional would be a severe blow to efforts to use bundled payments to improve care delivery in orthopedics and cardiac care, and to the chances for bringing bundled payments to scale nationally in the coming years.
Gronniger received funding from the American Medical Association unrelated to this article. Other than this assistance, none of the other authors received financial support from any firm or person with a financial or political interest in this article.
[1] The prospective payments systems Medicare uses for inpatient and outpatient services are arguably bundled payments relative to older payment arrangements based on individual items and services. For purposes of this paper, however, we focus on arrangements that span an entire episode of care over a period of time measured in months rather than days and that cover the services of multiple providers of care.
Authors








Commentary
How should the Trump administration handle Medicare’s new bundled payment programs?
April 10, 2017