As the coronavirus crisis continues, economic pressure and existing health systems challenges have aggravated disparities between the rich and poor in health care access and use. India’s experience is especially instructive, and not just because of its current difficulties in managing the exigencies related to COVID-19-related immunization, infections, and hospitalization.
Since 2005, over 270 million people in India have escaped poverty. However, COVID-19 and ongoing demographic and epidemiological transitions threaten to reverse this progress. While the government introduced major health reforms such as the National Health Mission (2005) and Rashtriya Swasthya Bima Yojana (RSBY, 2008) to cater to the needs of the poor, underfunded public health has struggled to meet the changing needs of people. Government health spending was only 1.17 percent of India’s GDP in 2016, a lower share than the low-income country average (1.57 percent).
By 2018, 62.8 percent of people did not have health insurance. Most households shoulder the burden of health care costs, with out-of-pocket expenses comprising 58.7 percent of total health spending. Furthermore, 1 in 5 households experiences catastrophic or impoverishing health expenses. Although RSBY—a publicly funded health insurance scheme for households below the poverty line—represented a big step toward universal health care, it grossly underperformed due to a low reimbursement ceiling, a limit of five enrollees per household, exclusion of outpatient care, and low enrollment. In addition, India’s decentralized health governance gives rise to the fragmentation of insurance schemes, contributing to systemic inefficiency and inequity.
The ambitious plans for the Pradhan Mantri Jan Arogya Yojana
A decade after the launch of RSBY, the government unveiled Ayushman Bharat, a national health initiative with a two-pronged approach. First, it called for the operationalization of 150,000 health and wellness centers by the end of 2022; these would serve as hubs for comprehensive primary health care. Second, it established the Pradhan Mantri Jan Arogya Yojana (PM-JAY), an insurance scheme that would cover secondary and tertiary health services for poor and vulnerable communities.
A recent review of PM-JAY by the Public Health Foundation of India and Center for Policy Impact in Global Health, Duke University found the following successes:
- Wider population coverage. Recognizing the limitations of RSBY, PM-JAY aims to cover an expanded beneficiary base of 107.4 million households with no cap on age, gender, or family size. Eligibility is not based strictly on income, meaning that coverage is extended to other vulnerable groups as well. Since the scheme’s launch in September 2018, more than 150 million beneficiary cards have been issued and nearly 18 million hospital admissions covered.
- Better benefit package and portable services. PM-JAY offers a significantly higher annual maximum of 500,000 rupees ($6,670) to beneficiary households. Over 125,000 people have availed “portable” services—a feature that entitles enrollees to PM-JAY benefits at any empaneled hospital in the country, regardless of home state—showing that the scheme has bridged gaps for those who cannot access the care they need locally.
- Stronger financial risk protection. Together, high value claims—those greater than 30,000 rupees ($400)—make up 41 percent of total claim payout, suggesting that PM-JAY has helped people get care that would have previously been out-of-pocket or catastrophic health expenses.
The implementation of PM-JAY marks the government’s commitment to the well-being of the most vulnerable populations and more broadly, to advancing universal health care in India. Despite impressive achievements in its first two years, PM-JAY faces serious challenges in equity, quality, effectiveness, and sustainability:
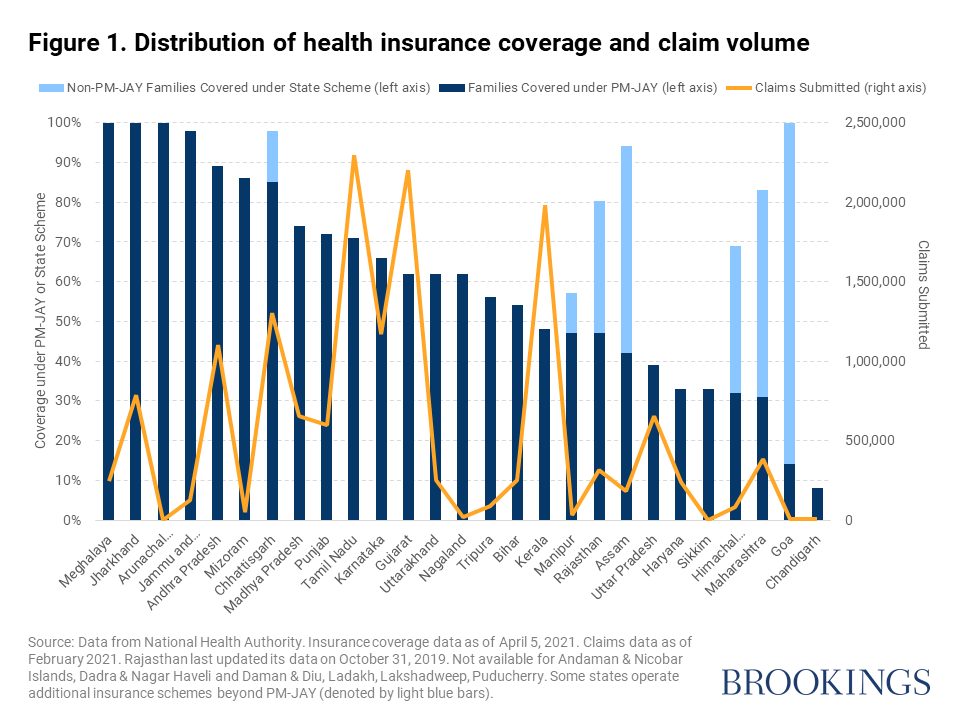
- Decentralized and inequitable implementation. While PM-JAY is a national initiative, its implementation is fully delegated to the states. With no overarching mechanism to address resource gaps, PM-JAY enrollment and service utilization are concentrated in wealthier states while poorer states are left behind (Figure 1).
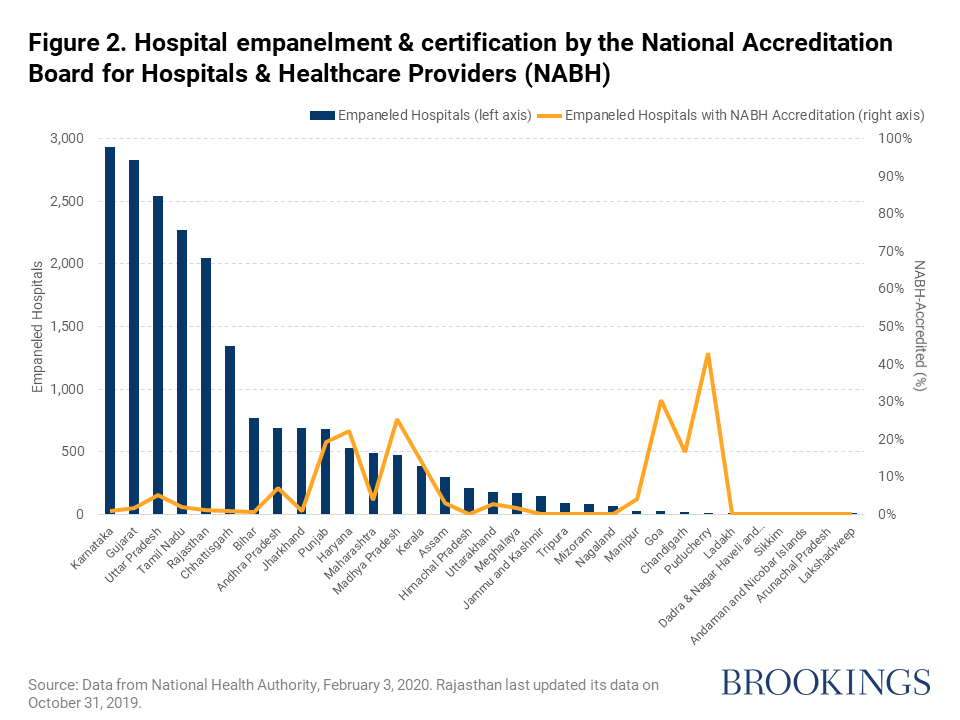
- Unbalanced provider quality and empanelment. Lack of public infrastructure and low-quality public health care have been long-standing problems in India. Under PM-JAY, states with higher poverty rates and disease burden see less empanelment and accreditation of hospitals. Overall, certification by the National Accreditation Board for Hospitals and Healthcare Providers is limited across all states, which raises quality concerns (Figure 2).
- Neglected outpatient and preventive services. Like its predecessor RSBY, PM-JAY does not cover outpatient care, which contributed to about 60 percent of India’s out-of-pocket expenses in 2016. In addition to not effectively minimizing out-of-pocket burden, PM-JAY’s exclusive focus on hospitalization favors reactive services and may shift care-seeking behavior away from cost-effective preventive care.
- Concerns about financial sustainability. Although the high service utilization under PM-JAY is promising, it also threatens the scheme’s sustainability. At the current rate of hospitalization, a 2019 report predicts that if PM-JAY were to successfully cover all target beneficiaries, its operating cost would significantly exceed its budget allocation. As vaccination rollout progresses and the cumulative COVID-19 caseload in India surpasses 17 million, the already-tight government budget for health is stretched even further. In 2020, India’s gross domestic product was estimated to contract by 8 percent, the largest drop in 70 years. Even with the proposed doubling of the next health budget, the long-lasting consequences of the pandemic put the financial sustainability of PM-JAY on edge more than ever.
What to do now
Looking ahead, the government of India has to consider further reforms to advance its universal health coverage ambitions. The most important areas are financing, costs, substitution, and quality.
- The financial sustainability and success of PM-JAY is related to the availability of funds required for implementation, as well as the willingness of the government to meet large-scale budget commitments and competing priorities created by the pandemic.
- In the longer term, rationalizing input costs through health technology assessments, exploring cross-subsidization and pooling across existing public health insurance schemes, and strategic purchasing to reduce wasteful spending can improve sustainability.
- While PM-JAY can help address financial shocks from large, one-time hospital expenses, it is crucial to avoid the substitution of primary care, which may inflate health spending. Out-of-pocket expenses on outpatient care, especially medicines, must be addressed by exploring integration with the PM-JAY benefits package. Furthermore, it is important to streamline referrals between health and wellness centers and PM-JAY facilities.
- Finally, quality of care is critical to the success of PM-JAY. Since most of India’s health system is privatized with loose regulation, it is important to strengthen state-level capacity to empanel and regulate private providers. Investing in health systems at the facility level is another key approach to ensuring equitable service access and delivery across rural-urban and rich-poor divides. More broadly, initiatives such as the National Digital Health Mission can also improve data management and transparency.
Related Content


Authors





Commentary
Early lessons from India’s health insurance scheme, Pradhan Mantri Jan Arogya Yojana
April 29, 2021