Universal health coverage (UHC) garners global support, as reflected in the UN Sustainable Development Goals and WHO global priorities. Yet, despite increased domestic financing for health and in spite of loads of evidence about the impact of increased spending on health and economic productivity, countries continue to under-invest in health care. Health spending in low-income countries (including aid and out-of-pocket spending) averaged about $19 per capita in 2016—less than one-fifth of the estimated $100 cost per capita for essential primary care coverage alone. Not only are domestic finances, donor aid, and out-of-pocket spending falling way short of covering cost, the gap between low-income and high-income countries in public spending on health care as a proportion of GDP is actually growing.
At the same time, there are big gaps in the quality of coverage. Many countries that nominally provide universal health coverage have serious access problems and inequalities. They also fail to exploit many opportunities for improving outcomes. Several recent studies, including reports by the US National Academy of Medicine and a special Lancet Commission, found widespread inefficiencies in care, leading to trillions of dollars in productivity losses annually in low- and middle-income countries. Millions die every year from treatable conditions. These problems lead many people—especially lower-income individuals—to pay for care, often for fee-for-service treatments of questionable value, from providers unconnected to publicly funded hospitals and clinics.
Closing this spending and health care gap through public finance and donor funding is becoming harder, not easier. Aging populations, the growing burden of chronic disease, and the potential for many more (at least initially, more costly) life-improving medical technologies present escalating threats to the financial sustainability of health systems. It is time to radically reconsider the mechanisms for getting to the goal of universal health coverage. This shift will require rethinking the role of the private sector in achieving universal health coverage and a new level of private sector leadership from both non-profit and for-profit organizations.
Innovations in care and genuinely integrated finance
Our analysis points to the need to promote low-cost innovation and aggressive integration of public and private finance.
First, achieving the goals of improved population health and financial sustainability will require new models of paying for health services and technologies that deliver better value for money. These new models will depend on encouraging low-cost innovation in delivery supported by private capital. Where universal health coverage policies leave out the private sector, UHC initiatives fail to deliver services reliably and efficiently. But where governments have created paths for private entities to be integrated into national coverage goals and be accountable, there are examples of successful health innovators. These initiatives are not yet scaled, but they have generated reliable evidence on payment and other reforms to promote innovation in efficient technologies and care delivery.
A few examples: Possible Health has worked with the government of Nepal to establish a community-based primary care system in rural regions for around $15 per person per year. With support from some Indian states to enhance access to high-quality cardiac services, Narayana Health, a for-profit network of 24 hospitals treating over 2 million people every year, has driven down the cost of cardiac surgery to less than $2,000. In Mali, Muso has implemented a community-based,person-centered model that proactively identifies at-risk individuals and delivers longitudinal care, leading to a significant reduction in child mortality. These models pay private health care providers for results at the person and population level, but they have not yet been widely implemented. It is time to scale them up.
Second, private initiatives can be better integrated with public spending. Separate public and private systems mean private resources are not being leveraged to close access and quality gaps. Poorer people need bigger subsidies to afford the higher-quality care preferred by those with more ability to pay. For example, Muso receives public subsidies to deliver a coordinated set of benefits to low-income individuals at no out-of-pocket cost. To the extent that publicly supported systems demonstrate value—timely and better care—they may also attract richer people. But many public systems in low- and middle-income countries are not integrated with private sector financial support to provide resources to benefit those who currently lack access or the ability to pay for better care. Our experience indicates that this can be changed.
Three ways to increase investment and innovation
Three changes are needed to achieve effective promotion of private innovation and investment; leveraging of private, voluntary spending on health services with public sector spending for better integrated care; and closing of the funding and quality gaps that are meaningful for universal health coverage.
1. Shift from paying for services to paying for outcomes
Countries at all income levels have stated their desire to implement “value-based care” through payment and regulatory reforms. Global leadership communities such as the World Economic Forum, OECD, G-20, among others, are supportive of this shift. Yet, most countries still pay for and organize health care around providers and services, not around the outcomes that matter to people. For all the United States’ efforts to move to “value-based” care, most payments are still based on the volume of services provided. The SDG target related to health care access still focuses on coverage of key services, not whether those or other innovative services are of high-quality or being put together effectively in practice for each person covered to achieve the SDG population health goals. The variation in quality and access across systems shows that paying providers for traditional service delivery is not sufficient for meeting UHC goals.
To be sure, reforms toward payment for health rather than service are difficult to implement. In 2012, for example, Ghana piloted a model to gradually shift provider payments from fee-for-service and hospital diagnosis-related groups (DRGs) to per-person payments. The government faced resistance including boycotts by private sector providers, and financial and operational obstacles in implementing the reformed care models. But there is now a better understanding of the capacities and changes needed to support local capacity building for value based-care, beyond traditional pay-for-performance or results-based financing programs.
In shifting to person-focused payments, policymakers should have in mind a progression of feasible value-based care goals and reliable indicators that public money is promoting these objectives. This approach includes identifying priority outcomes by engaging local communities and providers, strengthening primary care to reduce risk factors, monitoring efforts using simple measures, and holding providers accountable. To encourage participation by local providers and new entrants, pilots can be used to identify new ways of organizing care. Typically, such models shift the focus away from institution-based care to personalized, digitally-enabled models that emphasize prevention and early, local, intervention.
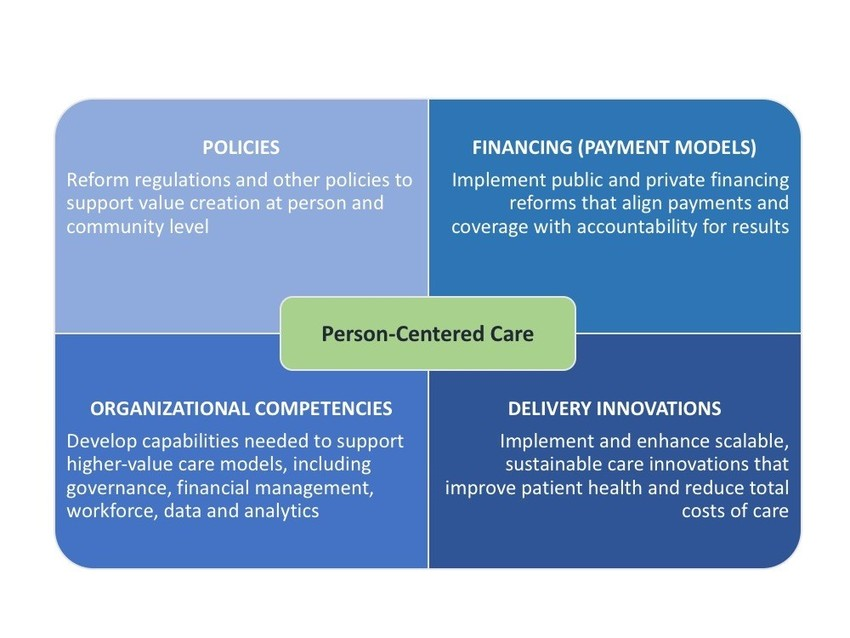
Image: Duke-Margolis Center for Health Policy
2. Build capacity for capturing and sharing data and track outcomes to encourage their use
The ability to capture and exchange key health and social data related to personal and community risk factors, treatment, patient experience, and outcomes leads to better decisions by patients, and is the foundation for monitoring results and rewarding organizations that are improving health. But data and measurement limitations remain serious barriers to faster progress toward value-based care, even in high-income countries that have made investments in health informatics infrastructure and standards. Are sophisticated information systems a bridge too far for poorer countries?
We are encouraged by the efforts of the World Health Organization (WHO) and the Institute for Health Metrics and Evaluation (IHME) to track disease burden in low- and middle-income economies. The International Consortium for Health Outcomes Measurement (ICHOM) and other entities also have established promising measures of outcomes of care for common conditions.
Success in value-based care reform requires extending data collection and measurement capacity to local populations as well as measures that can help in evaluating providers. Comprehensive electronic record systems are not needed; it is more important to find ways to obtain and use data for making initial improvements. With appropriate privacy protections, private companies experienced in obtaining, cleaning, standardizing, and sharing key consumer and business data—such as service utilization and satisfaction—can help governments build this capacity.
3. Scale and leverage effective value-based care models through subsidies
Income-based subsidies can enable individuals and populations to participate in value-based care models. Health care organizations eligible for such subsidies are chosen as an initial pilot with limited populations or small shifts from traditional financing. The main condition is that individuals and populations should be paid—at least in part—on the basis of accountability for outcomes and other conditions for aiding the shift to value-based care.
In countries where a growing middle class is increasingly buying private care, partial public subsidies for value-based care models can steer private investment toward value rather than fee-for-service models. Larger subsidies for people with lower-incomes can help them participate in the same care systems. Such subsidies could help unify public and private spending in support of more innovative care models and helping to drive private investment to develop and scale models that have shown evidence of improving health outcomes. The goal is to leverage the money that people with higher incomes spend on themselves to fund innovative capacity that can benefit the whole population, rather than driving private investments toward separate, often inefficient systems of care.
Leveraging the power of private providers
When facing regulatory conditions that enable sustainable business and growth around value-based care, private entrepreneurs have shown the ability to provide access and reduce costs in ways that are simply not achievable in traditional health financing models. Governments everywhere should be doing more to harness their energy and ideas. The World Economic Forum’s Global Coalition for Value in Healthcare can be a mechanism for accelerating the shift to value-based care and leveraging private resources to build public-private partnerships for better health care capacity that can benefit both rich and poor people.
Without private resources and resourcefulness, the essential goal of universal access to high-quality care and better health outcomes for all will remain difficult, even the wealthiest countries. For developing countries, it will remain out of reach and grow increasingly distant. Fortunately, many promising public-private initiatives are showing that it does not have to be this way.
Related Content



Related Books
Authors





Commentary
Achieving universal health coverage through value-based care and public-private collaboration
September 20, 2019